CHAPTER 2 Sports massage
Massage is one of the original core skills of physiotherapy (Copestake, 1917), which unfortunately fell from popularity because of the belief that it was ‘unscientific’. Thankfully, massage is making a re-emergence in the more fashionable guise of ‘sports massage’, both within physiotherapy and through the development of specialist massage therapists. A variety of massage types are commonly used, and a taxonomy of massage terminology by Dixon et al. (2007) described four main categories (Table 2.1).
Relaxation massage aims to create a feeling of wellness by moving body fluids (especially blood and lymph). This massage category includes both classical Swedish massage and Sports massage and is applied on healthy subjects. Traditional techniques in this grouping are highlighted in Table 2.2. Clinical massage may use these same techniques, but is applied to a pathological region of the body. Additional procedures such as trigger point release are often used to target pain. In clinical massage there may be considerable overlap with manual therapy which may be applied either to soft tissues (clinical massage) or joints (mobilization and manipulation). Movement re-education involves both massage and non-massage techniques. Where techniques such as Pilates, Alexander technique and Feldenkrais are used these are hands off procedures categorized as exercise therapy. Movement re-education using hands on techniques include tablework where the clinician assists or resists movement using proprioceptive neuromuscular facilitation (PNF) or MET (MET). These procedures may be preceded by relaxation massage to normalize muscle tone. Energy work capitalizes on the interaction between therapist and patient which always occurs during treatment. Now however the emphasis is to move blocked energy or ‘life force’ which is thought to flow within the body. In Chinese medicine this energy is Qi, in Ayerveda it is Prana. Massage in this category includes contact techniques such as Acupressure and Shiatsu and non-contact techniques such as Reiki and Healing.
| Effleurage |
| Unidirectional stroking movement travelling proximally |
| Petrissage |
| Soft tissue compression including kneading, picking up, wringing, rolling and shaking |
| Frictions |
| Small, deep circular or transverse movements at specific anatomical sites |
| Tapotement |
| Percussive actions including clapping, hacking, beating, tapping, shaking and vibration |
Massage techniques
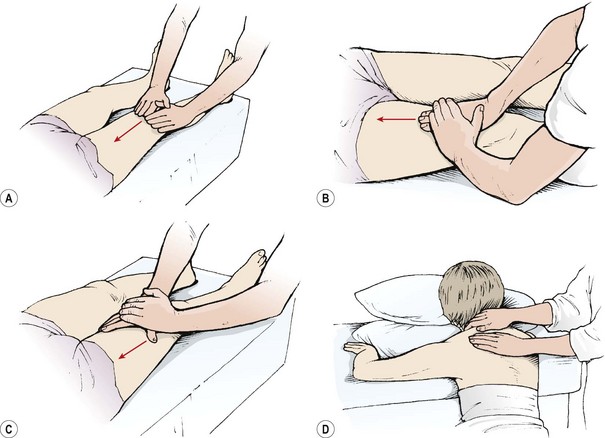
Effleurage
Two types of effleurage are used (Fig. 2.1). The first is a superficial stroking movement designed to produce a sensory reaction, either of relaxation (slow stroking) or stimulation (fast stroking). The second is a deep action aimed at assisting lymphatic and venous drainage. The tissue manipulation starts distally and proceeds proximally in the direction of the heart, for example, ‘knee to groin’ or ‘elbow to axilla’. The proximal portion of the limb is treated first to clear lymphatic and venous congestion. This will allow the tissue fluids mobilized by the distal massage to move against less restriction.
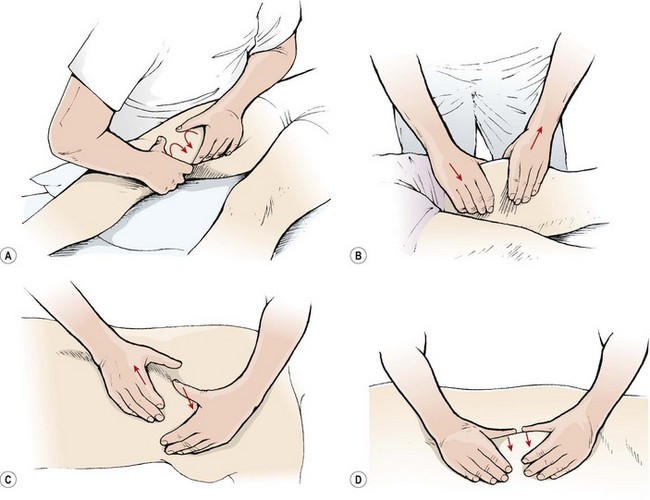
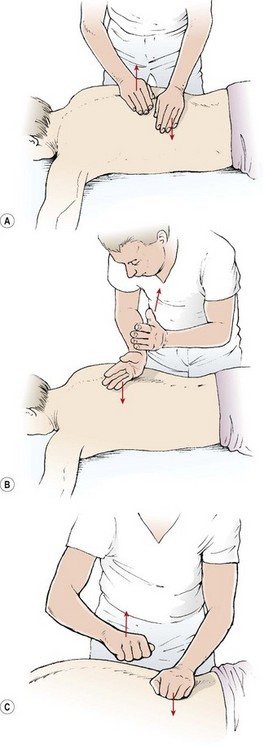
Petrissage
Various petrissage movements are used (Fig. 2.2). In each case the hands maintain contact with the skin and do not glide over the skin surface except when progressing from one area to another.
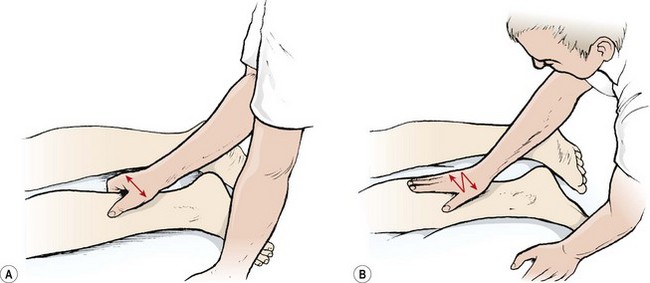
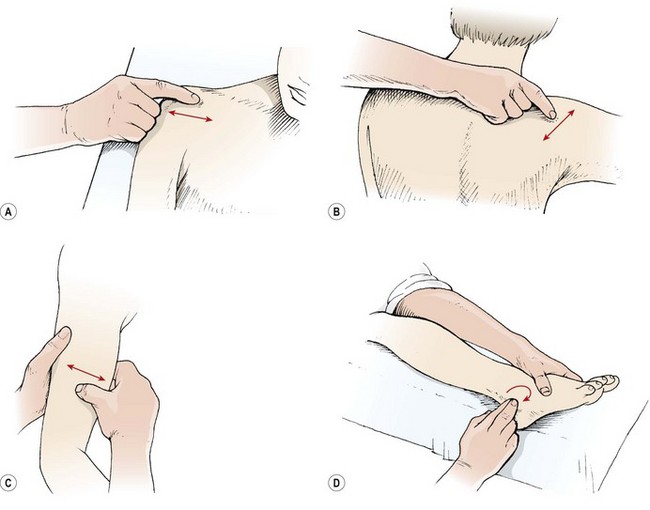
Frictional massage
With frictions, only the therapist’s fingers or thumbs are used to give an accurate, deep, soft tissue manipulation (Fig. 2.4). The fingers should be held locked but not hyperextended. With small areas, the first and second fingers are used overlapping as one unit. Larger areas may require the use of all of the fingertips of one hand reinforced by the other hand. The friction may either be circular or transverse.
Deep transverse frictions
Deep transverse frictional massage (DTF) is a specific manipulation technique pioneered by Cyriax (1941). The aim of the technique (Table 2.3) is to move the tissues with a view to improving function, and to induce hyperaemia and pain relief (Kesson and Atkins, 1998). DTF involves a transverse sweeping movement of the connective tissues which aims to discourage cross-link formation between collagen fibres. By applying shear and gliding movements in this way, tensile strength of the healing scar may be improved and adhesions reduced. Gentle DTF applied in the acute phase of healing could increase the rate of phagocytosis by inducing agitation of tissue fluid. In the chronic stage of healing, the therapeutic movement produced by DTF is said to soften and mobilize adhesions (Kesson and Atkins, 1998) in preparation for later tissue mobilization.
Table 2.3 Aims of deep transverse frictions (DTF)
Hyperaemia may be produced by DTF in the underlying tissues. Clinically, a red, raised area is seen on the skin as the technique is applied, and it is assumed that the same increase in regional blood flow occurs in the underlying tissues (Winter, 1968). The potential increase in the inflammatory response is required in chronic lesions but not in acute lesions. For this reason DTF, if used in the acute phase of injury, must be gentle and given over a shorter period to avoid hyperaemia production.
Treatment note 2.1 Saving your hands
Massage and manual therapy are powerful techniques; however, by their very nature they can cause considerable stress to the therapist’s hands. One study has shown that manual therapists are 3.5 times more likely to develop pain in the wrists and hands compared to non-manual therapists (Bork et al., 1996). Another study showed that therapists who used manual therapy were 7.7 times more likely to develop thumb pain and 4.0 times more likely to report wrist pain. Clearly this is an ‘at risk’ area and anything which can be done to reduce this risk is important.
Hyperextending finger joints
Many people have hyperextending finger joints (Fig. 2.5), meaning that, as they place pressure with the pad of their finger or thumb, the terminal digit is unstable and the joint extends further than normal, stressing both the ligaments and the muscles in the finger. In order to prevent this, both deep transverse frictional massage and joint mobilization techniques should be carried out with other parts of the hand.


Mobilization procedures can be carried out using the pisiform bone of the hand (Fig. 2.6). This small bone has approximately the same area as the thumb, and pressure can be placed through the straight wrist and carpal bones directly onto the pisiform itself. Where this area is too large, a plunger (Fig. 2.7) can be used. These come with a variety of different sized heads to correspond to different treatment areas.



For transverse frictional massage, the elbow may be used on large joints (Fig. 2.8). Because the elbow has a tendency to slip, it should be supported using the web of the finger and thumb of the opposite hand. Where direct digital pressure is needed over a period of time, for example deactivating trigger points deep within a muscle, a ‘knobber’ is useful (Fig. 2.9). This is a plastic device with a variety of different shaped balls on the end which can be used for greater or lesser pressure. These can be easily held in the hand to provide direct pressure to the trigger point. As an alternative, either a single knuckle or two knuckles may be used to provide greater or lesser pressure (Fig. 2.10).




Strain on the flexed wrist
Tendons around the wrist can become inflamed if the wrist is held in a flexed or adducted position for a long time. Where joint distraction movements are used (Fig. 2.11) it is important to pull through a straight angle of the wrist with the carpals and radius and ulna in line rather than flexed. This will ensure that the tendon sheath is not stretched and therefore compressed against the tendon itself. In addition, when using the thumb for manual therapy, again it is important that the wrist is in its neutral position and you avoid stretching the thumb tendons over the radial styloid.
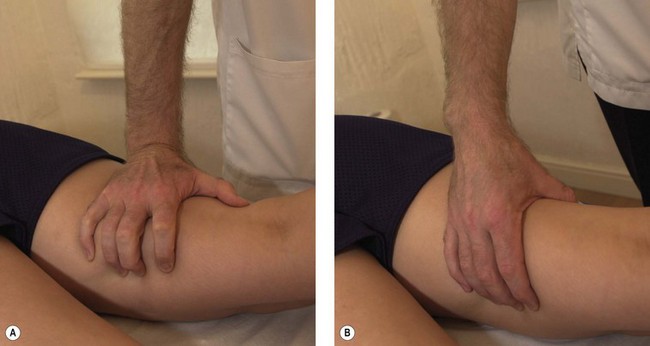
Figure 2.11 Avoiding stress on the wrist and hand. (A) Poor wrist and hand alignment. (B) Corrected.
The pain reduction seen with DTF may result from the massage acting as a noxious stimulus (counter-irritant) through mechanoreceptor activity. This would explain why DTF used aggressively gives better pain reduction than DTF given lightly, as the more aggressive approach will cause greater mechanoreceptor stimulation, which has been shown to increase pain suppression (Bowsher, 1988). Pain relief seen clinically is often fairly long-lasting, and a study by de Bruijn (1984) showed pain relief for up to 48 hours following DTF of 5 minutes maximum.
Restoration of function is often the most striking effect of DTF. On reassessment, range of motion is usually significantly increased and muscle contraction more easily performed. Kelly (1997) confirmed this in a study looking at 46 subjects who showed an increase in force of muscle contraction and an increased range of dorsiflexion after DTF of the gastrocnemius muscle.
DTF technique
DTF is performed with the skin of the patient and the finger(s) of the therapist acting as a single unit. A number of hand positions may be used to maximize the force applied to the tissues but minimize the stress imposed on the practitioner’s hands (Fig. 2.12). The action demands great anatomical accuracy and must be of sufficient depth and sweep to affect the desired tissues. The point at which the DTF is applied corresponds to the lesion in the tissues rather than the painful point, as pain is often referred away from the original site of injury.
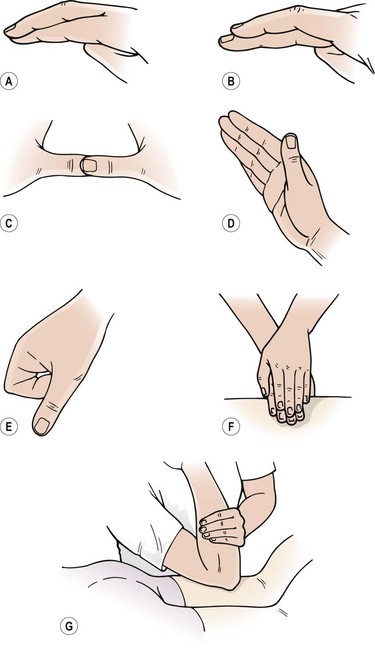
Figure 2.12 Hand positions for deep transverse frictions (DTF). Modified from Kesson and Atkins (1998). (A) Single finger. (B) Reinforced finger. (C) Reinforced thumb. (D) Knife edge of the hand. (E) Single knuckle. (F) Reinforced finger pads. (G) Elbow.
Tapotement
For stimulating tapotement the hands are relaxed, and follow each other in a succession of alternating movements. With clapping, the wrists are flail and the cupped hand strikes the body creating a hollow (rather than slapping) sound. Hacking involves striking the skin with either the ulnar border of the hand (severe) or the back of the tips of the fingers by using a pronation/supination movement of the forearm (mild). Beating or pounding is performed with the ulnar border of the semi-closed fist and tapping with the fingertips. The percussion techniques are used over bulky muscle areas but must avoid bony areas (spine of the scapula, patella) as these will be painful if struck (Fig. 2.13).
Massage medium
Massage can require both slip (lubrication) and grip (friction), depending on the particular technique being performed. Grip media include talc or corn starch, while lubricants may be oils, creams or lotions. Where one technique progresses on to another, practitioners may often find themselves wanting one medium while using another. The functions of grip and slip media are shown in Table 2.4. It must be noted, when using oil, that patients may be allergic to nuts and suffer anaphylactic shock. Peanuts are the most common nut allergen with approximately 1 in 500 of the population affected (Demain, 1996). Traditionally used arachis oil is derived from peanuts, and oils such as almond are obviously nut based.
Table 2.4 Function of media used in massage
| Lubricant (slip) | Friction medium (grip) |
|---|---|
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
