Fig. 14.1
Sternal lift. This maneuver is performed standing with the trunk and knees slightly flexed (a). The patient is instructed to extend the hips and trunk and retract the scapulae without moving the glenohumeral joint (b)
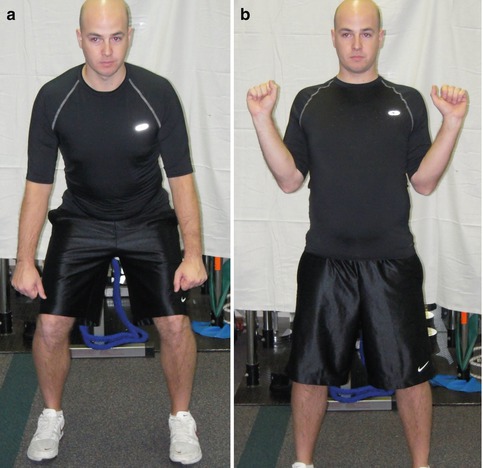
Fig. 14.2
Robbery exercise. The robbery maneuver begins with the knees and trunk flexed and the arms held away from the body (a). The patient is instructed to extend the hips and trunk and to “place the elbows in the back pockets,” holding this final position for 5 s (b)

Fig. 14.3
Lawn mower exercise. The lawn mower begins with the hips and trunk flexed and the arm slightly forward elevated (a). The patient is instructed to extend the hips and trunk, followed by rotation of the trunk to facilitate scapular retraction (b)
Excessive scapular protraction does not allow optimal rotator cuff activation to occur. Rotator cuff strength can increase when the scapula is stabilized and retracted. The muscles responsible for performing scapular retraction can help control scapular protraction through eccentric control. When optimized, these muscles can properly maintain scapular stability thus decreasing excessive protraction with arm movement. For this reason, the early phases of training should focus on scapular strengthening in an attempt to restore normal scapular kinematics rather than placing an early emphasis on rotator cuff strengthening as performed in more traditional rehabilitation protocols.
14.6.4 Early Closed-Chain Implementation
Kinetic chain-based rehabilitation activities have been grouped into open and closed chain. Typically, when soft tissue is pathologic, closed-chain exercises are implemented early in the rehabilitation process. There are three components which make usage of closed kinetic chain exercise advantageous in early rehabilitation. First, the exercise environment can be controlled. This allows the focus to be taken away from the arm as an integrated unit with high dynamic demands and place it in a stable, axially loaded, static setting. Second, closed-chain exercise is ideal for working “at” specific ranges of motion compared to working “through” a range of motion. Finally, closed-chain exercise allows the rotator cuff and scapular musculature to be unloaded by decreasing the amount of force generated and stress applied to the involved soft tissue. These types of exercises are best suited for reestablishing the proximal stability and control in the links of the kinetic chain such as the pelvis and trunk. Open-chain exercises, which generate greater loads in comparison to closed-chain activities, should be utilized later in rehabilitation programs due to their increased demand on the soft tissue due to the longer arm levers these exercises require.
The rationale behind the closed-chain framework is to maximize the ability of the inhibited muscles to activate. This involves placing the extremity in a closed-chain position, emphasizing normal activation patterns, and focusing on the muscle of interest by deemphasizing compensatory muscle activation. For example, if a patient presents with shrugging during arm elevation, then it can be assumed that the lower trapezius and/or serratus anterior is not working effectively enough during the dynamic task. A closed-chain exercise such as the low row should be utilized because the short-lever positioning in conjunction with the pelvis and trunk acting as the driver facilitates lower trapezius and serratus anterior co-activation which decreases the activation of the upper trapezius (Fig. 14.4). This is the normal muscle activation pattern for scapular retraction and depression. Once the normal activation pattern has been restored, then more challenging isolated exercises can be employed.

Fig. 14.4
Low row exercise. The patient is positioned standing with the hand of the involved arm against the side of a firm surface and legs slightly flexed (a). The patient should be instructed to extend the hips and trunk to facilitate scapular retraction and hold the contraction for 5 s (b)
14.6.5 Work in Multiple Planes
Strengthening and stabilization should begin by emphasizing work in successful planes and then progress to deficient planes. Clinicians should avoid the use of single planar exercises which isolate specific muscles or specific joints. Greater isolation should be utilized in the later stages of the rehabilitation protocol. During the early phases, emphasis should be placed on achieving successful positions, motions, and muscle activation sequences. In this manner, normal physiologic activations are restored, which lead to restoration of normal biomechanical motions.
Most activities, whether they are sports-related or normal daily movements, occur in the transverse plane. Therefore, the transverse plane should be exploited particularly in the early phases of rehabilitation. The protocol should progress to more unilateral planes as normal scapulohumeral kinematics are restored. Exploitation of the transverse plane and exaggeration of trunk motion help accentuate both scapular retraction and protraction. By forcing proximal stability, the hip and trunk muscle activations, which have been demonstrated to precede arm motion, will be more effective during a specified task (Fig. 14.5). In addition to generating and transferring energy to the distal segments, this component of rehabilitation allows the utilization of the stable base for arm motion and forces the lower extremity and core to drive the arm (Figs. 14.6 and 14.7). Rehabilitation programs should attempt to encourage stimulation of proper proprioceptive feedback as well, so the patient can return to their desired level of function.

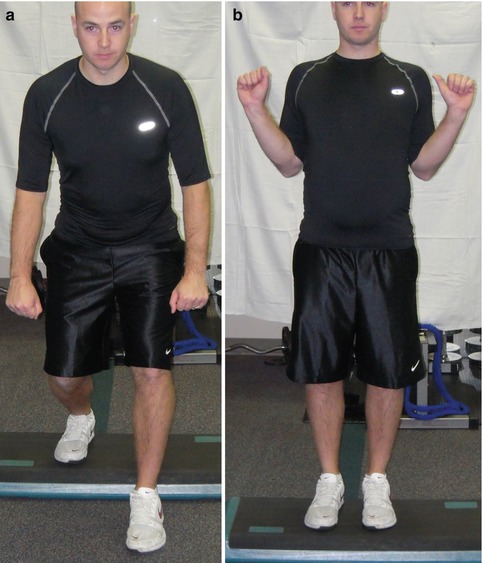

Fig. 14.5
(a, b) Lawn mower with lateral step. By adding the step, the patient is forced to utilize the hip abductors making the exercise more functional
Fig. 14.6
(a, b) Robbery exercise with posterior step. Utilizing the step allows the lower extremity to drive the upper extremity
Fig. 14.7
(a, b) Low row with posterior step. The posterior step back requires hip and trunk extension which facilitates scapular retraction and depression
14.7 Advantages/Pitfalls/Complications
The primary advantage of considering scapular function as a component of overall shoulder function is that scapular considerations allow the clinician to employ a comprehensive approach of assessment and treatment. Such an approach helps to eliminate placing sole focus on the site of symptoms and instead direct attention toward potential causes of symptoms and/or dysfunction. Adhering to the kinetic chain model of function is also helpful in appreciating the influence the scapula can have on arm function because of the understanding of segmental motion and energy transfer.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


