Radius and ulnar diaphyseal fractures
Anatomy and biomechanics of the forearm
Principles behind surgical fixation
INTRODUCTION
Diaphyseal forearm fractures are uncommon in the elderly. Most fractures are treated operatively, especially if both the ulna and the radius are fractured. Stabilization with plates and screws enhances union, provides better alignment, allows immediate functional use of the arm and is safe for most open fractures. In the elderly, a locked plate might be useful when the plate extends into the metaphysis. It is not clear that intramedullary nailing can accurately restore the radial bow and control rotation in comminuted fractures. Bone grafting is not necessary when comminution is bridged and periosteal and muscle attachments are preserved. Complications such as infection, nerve damage, malunion and nonunion from operative treatment are uncommon.
EPIDEMIOLOGY
Diaphyseal fractures of the forearm usually result from an axial load applied to the forearm through the hand.1 The incidence and prevalence of diaphyseal forearm fractures decrease with age. The average age of an adult with a forearm fracture is 35 years.2 Court-Brown and Caesar studied a population of over 5900 fractures and noted a prevalence of 24% in individuals over 50 years of age, 13% in those over 65 years of age and 12% in those over 75 years of age.2 Among various categories of patients grouped by age and sex in patients aged 60 or greater, Singer et al. reported an incidence of forearm diaphyseal fractures ranging from no fractures to 4.3 fractures per 10,000 population per year (Table 25.1).3
EVALUATION AND DIAGNOSIS
Diaphyseal fractures of both forearm bones are usually obvious due to the inherent instability created by the injury. Individual fractures of the radius or ulnar may be less obvious. As with any skeletal injury, physical examination should include the entire extremity, paying particular attention to the joints and soft tissues as well as the bone. Look for skin lacerations indicating an open fracture. When only one forearm bone is fractured, evaluate the proximal and distal radioulnar joints. It is also important to check the neurovascular status of the limb by documenting pulses and neurologic function distal to the injury. Examination of the surrounding soft tissues is important not only to rule out concurrent acute issues such as compartment syndrome but also to judge appropriate timing for surgical intervention.
Radiographs are usually sufficient for the evaluation of diaphyseal forearm fractures. Computed tomography (CT) scans may be used on occasion to evaluate radioulnar joint alignment.
ANATOMY AND BIOMECHANICS OF THE FOREARM
The proximal radioulnar joint is stabilized by the annular ligament, while the distal radioulnar joint is stabilized by the triangular fibrocartilage complex (the dorsal and volar radioulnar ligaments in particular), the wrist capsule and the interosseous ligament (perhaps a distal band in particular). These structures have the potential to be damaged with forearm trauma and are at particular risk when only one forearm bone is broken.
Table 25.1 Incidence of diaphyseal forearm fractures per 10,000 population per annum by age and gender
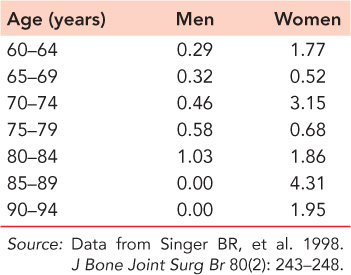
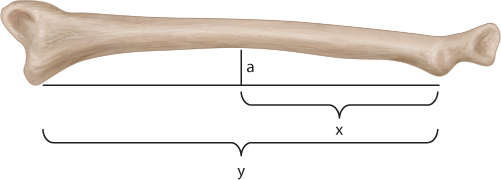
Figure 25.1 Illustration showing measurement of radial bow. Maximal radial bow is located at position ‘a’. Location of maximal radial bow is equal to x/y times 100.
The ulna is a relatively straight bone around which the bowed radius rotates. Full pronation and supination depend on the bow of the radius away from the ulna. This bow allows for clearance of the ulna and the forearm muscles (Figure 25.1).4 The oblique grouping of fibres which connect the two bones is referred to as the interosseous ligament. This broad ligament functions as a longitudinal support of the radius and also prevents separation of the two bones.
Disruption of the bones at particular levels may result in specific deformities due to soft tissue attachments. With proximal third fractures, the biceps and supinator muscles flex and supinate the proximal fragment, while the distal fragment is pronated by the pronator teres and the pronator quadratus. Fractures involving the middle third of the forearm have the supinator, biceps and the pronator muscles maintaining the proximal fragment in a neutral position, while the pronator quadratus pronates the distal fragment. The brachioradialis dorsiflexes and radially deviates the distal segment in distal third fractures while the pronator quadratus, wrist flexors and extensors and thumb abductors can add additional deformities depending on the location of the fracture.5 Understanding these deforming forces enables the physician to treat fractures amendable to closed treatment with the forearm supinated for proximal third fractures, neutral for middle third fractures and pronated for distal third fractures. This knowledge can also help facilitate open reduction.
PRINCIPLES BEHIND SURGICAL FIXATION
Strain is defined as the change in the length of a fracture gap under a load divided by resting length of the fracture gap, also known as the percentage of a deformation of a material or zone. Primary bone healing occurs when the strain is kept to less than 2%.6 A strain of 2–10% has been found to be ideal to induce secondary healing through callus formation.7 Both bone forearm fractures that do not involve comminution can be treated with rigid fixation using compression. This method creates a minimal strain environment allowing direct primary bone healing. For transverse fractures the plate is slightly pre-bent and placed on the tension side of the fracture so that the far cortex compresses first (Figure 25.2).8 For oblique or spiral fractures, interfragmentary compression screws can be placed outside the plate and then supported with a neutralization plate.
Fragmented forearm fractures are managed with bridge plating, which relies on secondary bone healing (healing by callus) (Figure 25.3). If there is more than a simple butterfly fragment, it is better to not perform precise reduction of each fragment. Rather it is important to preserve the periosteal sleeve and muscle attachments and restore length and alignment. The plate maintains alignment by providing relative stability, and higher strain, leading to healing by callus (Figure 25.4).
Plates with screws that lock to the plate are not usually necessary or helpful for diaphyseal fractures because diaphyseal bone maintains good quality even in the later years. Cadaveric studies looking at plate and screw constructs have found that the length of the plate used is more important than the number of screws used. Sanders et al. found that with four-point mechanical testing, longer plates with two screws in the outermost holes and two screws in the inner most holes were stronger than a six-hole plate with six screws used when tested in medial-lateral and tension band modes.9 When a fracture is relatively proximal or distal and when important screws for fixation will be in the metaphysis, locked screws can help gain better fixation of osteoporotic bone in the elderly.6 In these circumstances the locked plates can enhance fracture fixation where fracture configuration or bone quality do not provide sufficient screw purchase to achieve the plate-bone compression necessary to minimize the gap strain with unlocked plate screw constructs (Figure 25.5).6
Studies looking at angular malalignment have found that forearm rotation is limited with angulation of the ulnar or radius greater than 20 degrees.10 Restoration of the normal bow of the radius helps maintain forearm rotation and grip strength. The radial bow is assessed on an anteroposterior (AP) radiograph with the forearm in neutral rotation, the shoulder abducted 90 degrees and the elbow flexed 90 degrees. The bow is quantified by drawing a line from the radial tuberosity to the most ulnar edge of the distal radius. A perpendicular line is then drawn at the point of maximal radial bow with the length of this line then being measured (Figure 25.1).4 It can be helpful in comminuted fractures involving both bones to obtain radiographs of the uninjured forearm to help guide surgical treatment of the injured side. Determining the appropriate radial bow is essential to properly stabilizing the fracture for functional use of the extremity.
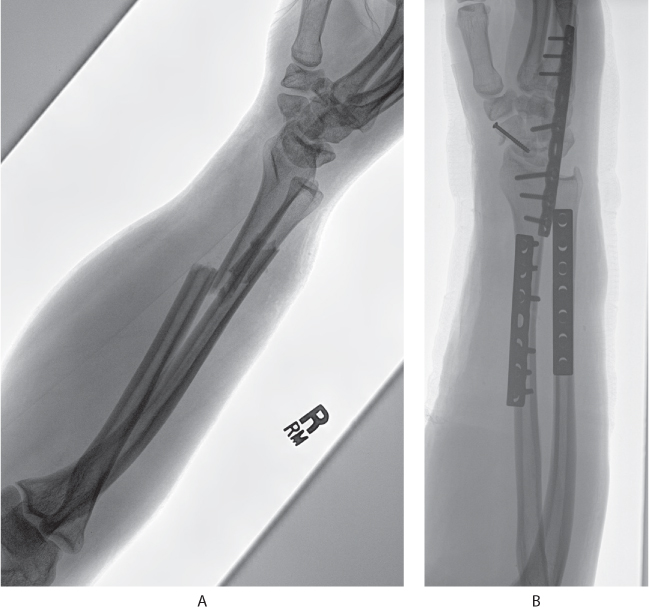
Figure 25.2 (a) Preoperative radiograph depicting transverse fractures of radius and ulna. (b) Postoperative radiographs showing the ideal method for treating transverse fractures with the plate slightly pre-bent and placed on the tension side of the fracture so that the far cortex compresses.
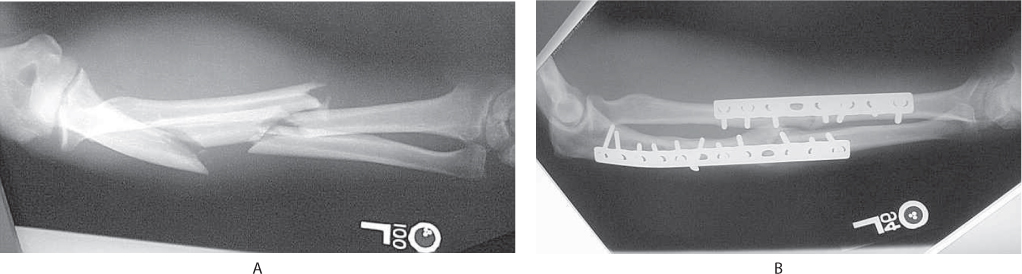
Figure 25.3 (a) Preoperative segmental both bone forearm fracture. (b) Bridge plate technique used to treat segmental both bone forearm fractures. Bridge plating relies on secondary bone healing.
MANAGEMENT
Initial and nonoperative management
Most diaphyseal forearm fractures in adults are unstable and benefit from splint immobilization for comfort prior to surgery. Because diaphyseal bone fractures and isolated radial shaft fractures are usually unstable there is little role for nonoperative treatment. Regaining length can be difficult, particularly if the patient has a muscular forearm, so surgery should be scheduled within a few days.
Isolated fractures of the ulna with fewer than 10 degrees of angulation and at least 50% apposition can be treated nonoperatively. Nonoperative treatment in a short arm cast or removable brace may be sufficient and it is used essentially to treat the symptoms associated with the injury (Figure 25.6). Sarmiento et al. have demonstrated that even with up to 50% displacement of the shaft, stabilization with a functional fracture brace with a good interosseous mold can maintain alignment and allow healing.11
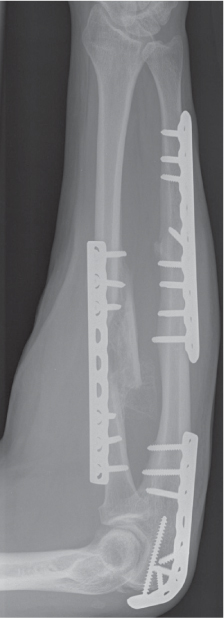
Figure 25.4 Bridging technique utilized to restore length rather than precise segmental fixation.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


