Preoperative assessment and care of the elderly
Major goals in the preoperative period
Unique physiologic considerations
Management of preoperative anticoagulation and thrombosis
INTRODUCTION
Like many other geriatric medical topics, preoperative assessment and care practices are heavily informed by the integration of geriatric principles with evidence extrapolated from other populations. There is a paucity of well-validated literature on preoperative risk assessment and management of geriatric surgical patients, and even less concerning the subset of patients undergoing urgent or emergent procedures, for instance following orthopaedic trauma. For these reasons, the existing literature in these areas can be best used as a starting point for practice recommendations and then further modified for the unique and varied physiologies and vulnerabilities of older adults.
The lack of explicit evidence-based guidelines for each preoperative clinical issue can be a source of frustration and skepticism for clinicians, especially for those hoping to access uniform and detailed algorithms for the preoperative assessment and optimization of fragility fracture patients. Despite this, centres using a standardized geriatric medicine approach to preoperative care have reliably demonstrated improved outcomes in mortality, length of stay and reduction in complications.1,2 and 3 This chapter focuses on the strategies used by many of these centers and describe the unique physiologic considerations of the geriatric trauma patient, medical, cognitive and functional status assessment, preoperative risk assessment, preoperative testing and medical optimization for surgery.
MAJOR GOALS IN THE PREOPERATIVE PERIOD
In contrast to patients undergoing elective procedures, the preoperative care for older adults with acute trauma is additionally focused on pain control and preoperative hemodynamic stability and avoidance of functional decline (Table 3.1). Early surgery is typically the most important means to achieve these goals, and the preoperative medical assessment needs to prioritize early surgery and early mobility over most other clinical issues. For these reasons, high performing geriatric fracture centers have implemented clinical pathways that emphasize timely transition to operative repair, even in highly comorbid or frail older adults. Many notable comorbidities warranting more intensive preoperative testing and consultation prior to elective surgery are not vigorously pursued in the urgent surgical setting.
UNIQUE PHYSIOLOGIC CONSIDERATIONS
The older adult is prone to exaggerated hypotension in the perioperative period.4 This is a predictable consequence of cardiovascular aging and often exacerbated by commonly used cardiovascular medications (including antihypertensive and antianginal medications) as well as opioid analgesic and other anaesthetic medications. The heart and vascular tree undergo significant losses in elasticity and compliance over time and result in secondary clinical problems including impaired ventricular filling, widened pulse pressure, diastolic hypotension and elevated atrial pressures. Even in patients without a demonstrated impairment on resting echocardiography, the older heart is less able to easily respond to blood loss, pain and vasodilation. The aging of the autonomic nervous and cardiac conduction systems also results in impaired neurocardioprotective reflexes, postural hypotension and limited ability to compensate for volume loss or vasodilation.5 Large drops in intraoperative blood pressure can be common and severe, even in patients whose preoperative blood pressure is normal or elevated. While this is well known in the anesthesia literature, it may be underappreciated by medical physicians and surgeons.
Table 3.1 Major goals of the preoperative period
Hemodynamic stabilization |
Pain control |
Perioperative risk assessment |
Timely preoperative optimization |
In addition, older adults are more prone to a number of serious and potentially conflicting perioperative complications, including excessive bleeding and thrombosis, agitated delirium and lethargy. While not the focus of this chapter, the initial preoperative plan is important to minimize the development of these common complications. Further discussion of postoperative complications can be found in Chapter 7.
Many fragility fractures occur in patients with multi-organ age and disease-related impairments, producing a general state of decreased physiologic reserve.6 This concept is useful as an overarching paradigm to explain the diversity of complications that can emerge in older adults, as well as to reinforce the central role of general strategies to minimize stress (including intravascular volume depletion), immobility and pain.
PREOPERATIVE RISK ASSESSMENT
For all but the most critically ill patients, the benefits of operative fracture repair (hemostasis, pain control, mobilization) will exceed the risks related to anesthesia and surgery. This is due both to advanced anesthetic and surgical techniques and to the excessive morbidity and mortality of the hip fracture patients in the absence of surgical repair. One of the major goals of the preoperative assessment is to estimate the risk of poor surgical outcomes, including cardiovascular complications, stroke and death. Patient specific risks can be roughly estimated with the careful and limited use of preoperative risk calculators.
Risk calculators
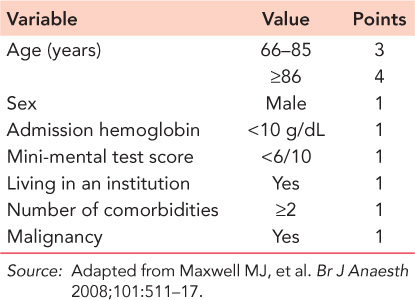
The Nottingham Hip Fracture Score7 is the best-validated instrument for predicting 30-day and longer outcomes in the hip fracture population and incorporates measures of comorbidity burden, functional status (type of residence), cognitive status (mini-mental test score) and key demographic factors (age, sex). Some elements (institutionalization, mini-mental test score) are not universally uniform across different international settings but likely can be approximated and remain useful for estimating perioperative risk and short-term outcomes (Table 3.2).
Table 3.2 Nottingham Hip Fracture Score
A number of additional calculators have been developed in an attempt to provide a reasonable estimate of serious complications in surgical patients; none are validated in older adults undergoing urgent orthopaedic surgery. Three calculators that were examined in the most recent American College of Cardiology/American Heart Association (ACC/AHA) guidelines include the Revised Cardiac Risk Index (RCRI),8 the Myocardial Infarction or Cardiac Arrest (MICA) calculator9 and the American College of Surgeons’ National Surgical Quality Improvement Project (ACS NSQIP) risk calculator10 (Table 3.3). Each calculator has strengths and weaknesses; the RCRI is by far the most common of these and has been incorporated into studies of older adults with hip fractures. Although they have outperformed the RCRI in initial studies, neither the MICA nor the NSQIP calculators have been well validated outside of a single center or cohort. While all three attempt to address procedure specific risk and comorbidity measures, the NSQIP and the MICA also incorporate a gross measure of functional status. The standard RCRI may be improved11 by removing the diabetes criteria and substituting a glomerular filtration rate of less than 30 mL/min for the original creatinine criteria (serum creatinine greater than 2 mg/dL). In light of these considerations, any of the three calculators will likely give a reasonable estimate of risk that can be further adjusted based on patient specific trajectory and reserve.
Biomarkers
Patients with elevated biomarkers (B-type natriuretic peptide and troponin assays) have been shown to have a significantly increased risk of perioperative morbidity and mortality,12,13 but the optimal ways to use these measures in this setting remain unclear. There is no evidence that treatment aimed at these biomarkers is helpful, and there is concern that abnormal findings may inappropriately delay surgery or prompt potentially harmful interventions (acute diuresis, antithrombotic treatment) in hemodynamically and hemostatically unstable patients. Further prospective studies will be needed.
Table 3.3 Risk assessment calculators
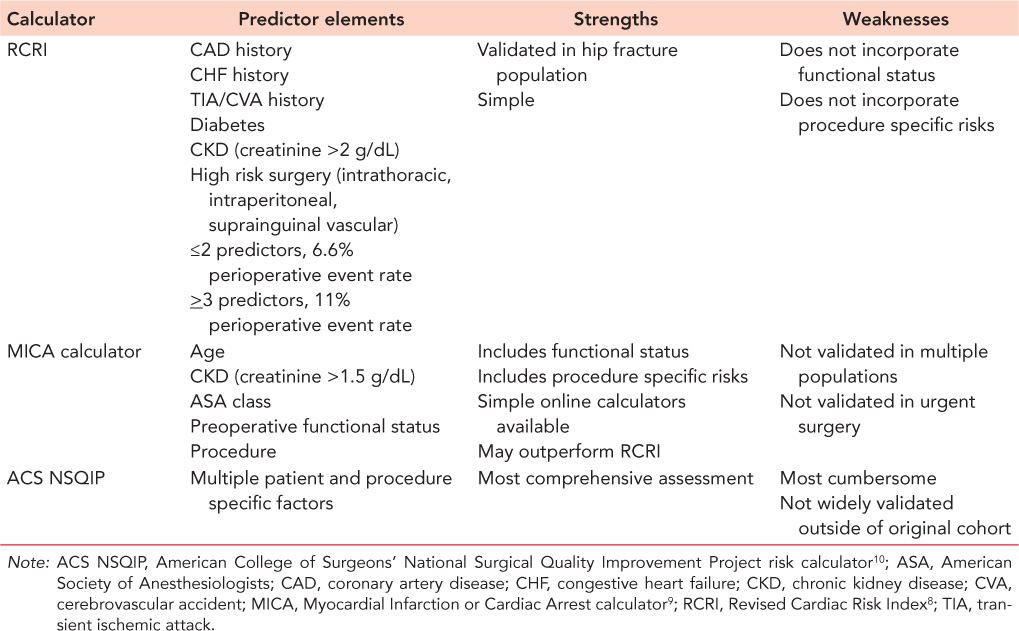
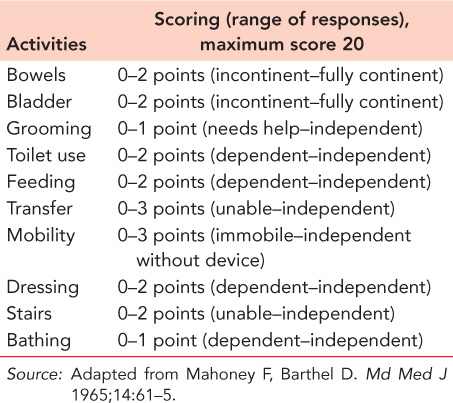
Table 3.4 Barthel Index of Activities of Daily Living
Other assessments of prognostic importance
Despite the historical emphasis on comorbidity scoring for estimating surgical risk, there has been increasing recognition that other assessments may also play an important role in correctly stratifying patients and predicting outcomes. These assessments aimed at functional status, cognition, exercise capacity and nutritional status may provide significant predictive ability, and, in some cases (nutrition), stimulate helpful interventions. Functional and cognitive impairments have long been recognized in geriatric medicine to predict outcomes including mortality,14 and measures of both function and cognition are beginning to be embedded in some preoperative risk assessments.
Functional assessments
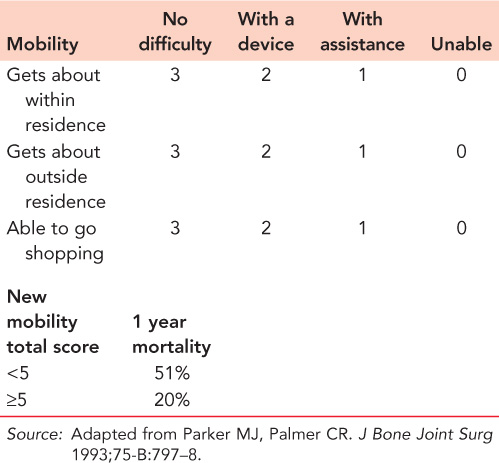
Although the details are beyond the scope of this chapter, functional dependence is often evaluated by activities of daily living (ADL) scoring (e.g. the Barthel Index) (Table 3.4).15 The Parker Mobility Score is a simple measure of function that has been derived and validated in the hip fracture setting and evaluated in multiple settings and for multiple important outcomes including mortality16 and postsurgical independence17 (Table 3.5).
Cognitive assessments
Impaired cognition is significantly associated with functional dependence and poor outcomes and by itself is often a marker of increased perioperative risks and postoperative dependency.18 Patients with a pre-existing diagnosis of dementia have a significant risk of mortality at 6 months. For patients without a pre-existing diagnosis, diagnostic assessment for dementia is often not possible during the preoperative period, in light of the high prevalence of delirium. In these situations historical features can often suggest underlying cognitive impairment; impairments in telephone use, handling of finances and medication self-administration best correlate with underlying dementia.19
Table 3.5 New Mobility Scale (Parker Mobility Scale)
Exercise capacity
Exercise capacity is used as a surrogate for functional capacity and physiologic reserve and has been incorporated into the ACC/AHA guidelines to distinguish between high and low risk patients, using a threshold of four metabolic equivalents of task (METs). Common activities that meet this threshold include walking up a flight of stairs, walking up a hill, walking on level ground at a minimum pace of 4 mph, or heavy housework (scrubbing floors, moving heavy furniture). For patients undergoing elective surgery, these guidelines suggest that patients who can perform this level of exertion do not require additional cardiovascular testing preoperatively.
Nutritional status
Malnutrition20 is highly prevalent in hip fracture patients and is suggested by low body mass index, low serum albumin or significant unintentional weight loss.21 It is independently associated with poor perioperative and postoperative outcomes and can further inform prognostication for older adults. Simple historical tools to identify patients with weight loss and routine albumin testing can both be incorporated into preoperative assessment practices.
PREOPERATIVE TESTING
In an attempt to minimize surgical delay, pain and delirium, the standard preoperative evaluation should consist of only essential radiographic studies, bedside clinical evaluation by medical, surgical and anesthesiology teams and basic serum blood work and electrocardiography. Observational studies suggest that excellent perioperative outcomes can be obtained with protocols that emphasize plain radiography of the fracture, hemoglobin levels and platelet counts, basic serum electrolytes and renal function and a resting electrocardiogram22 (Table 3.6). Additional studies to identify contributors to metabolic bone disease (calcium and phosphorus, parathyroid hormone, thyroid hormone, vitamin D levels) or help identify malnutrition (albumin levels) can be obtained preoperatively as well, although the results of these studies are not essential prior to proceeding to surgical fixation. Order sets and protocols for fragility fracture patients can help streamline this preoperative testing process and help minimize inappropriate variation in care.23
Bedside clinical evaluation remains the cornerstone of preoperative assessment and should be focused on the assessment of intravascular volume status and the rapid identification of the small numbers of active medical conditions that would warrant surgical delay, including acute pulmonary oedema, acute coronary syndrome, sepsis, unstable arrhythmias or acute stroke.
For most fragility fracture patients there is no demonstrated benefit to routine advanced investigations such as echocardiography, non-invasive cardiovascular stress testing or prolonged preoperative cardiac rhythm monitoring. Retrospective studies suggest that routine intensive cardiovascular testing, including routine echocardiography, results in significant surgical delay without any clinically important changes in management.24,25 In addition, the preoperative care teams should carefully avoid preoperative workup of otherwise stable chronic comorbidities (e.g. chronic renal failure, chronic stable coronary disease and chronic neurologic deficits); there is no known benefit to more intensive workup and consultation prior to fracture fixation. Other routine tests of uncertain preoperative impact include routine urinalysis, chest radiography and biomarker assays (BNP and troponin). The high incidence of asymptomatic bacteria in older adults (particularly women) can result in complications related to inappropriate antimicrobial use, and abnormal biomarker levels may prompt acute interventions that may promote hypotension, bleeding and surgical delay. Until there are better prospective data supporting routine use of biomarker assays in fragility fracture patients, these should be limited in this setting to symptomatic patients.
Table 3.6 Basic preoperative testing
Blood counts (hemoglobin, hematocrit, platelet counts) |
Serum electrolytes |
Renal function |
Resting electrocardiogram |
Plain radiography of fracture |
Metabolic bone studies (vitamin D, calcium, phosphorus, parathyroid hormone, thyroid studies) |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


