Distal tibial fractures
INTRODUCTION
As the proportion of elderly individuals increases due to longer average life expectancies, fracture incidence in this population is on the rise. In addition to decreasing bone mineral density (BMD), multiple explanations have been proposed for the increased incidence of fractures in the aging population including ‘frailty’, a condition defined by a diminished capacity to perform activities of daily living and often characterized by inactivity and weight loss.1 Other risk factors for osteoporotic fractures include vitamin D deficiency, malnutrition, chronic inflammatory conditions, physical deconditioning and poor balance.1
Although much less common than the classic fragility fractures of the proximal femur, pelvis, proximal humerus and distal radius, fractures of the distal tibia and fibula in the elderly most commonly result from similar mechanisms of injury – ground level falls. Measurements of BMD obtained from the tibial diaphysis and epiphysis have been shown to predict clinical fracture risk as accurately as BMD measurements obtained from the hip or lumbar spine, substantiating the fact that osteopenia and osteoporosis are manifest in the entire skeleton.2
EPIDEMIOLOGY
Although the majority of recent literature examining changes in the incidence of fragility fractures has focused on the classic fragility fractures described above, Court-Brown et al. have recently published a detailed epidemiologic analysis of fractures in patients 65 years of age and older.3 In this series of 4,786 fractures that occurred over 24 months of data collection, only 16 (0.33%) occurred in the distal tibia, representing an overall incidence of 8.2 per 100,000 population per year (3.9 in males and 11.0 in females). Of the 16 distal tibia fractures, 15 occurred as the result of low energy falls, and one occurred spontaneously (Court-Brown CM, personal communication). Unlike with many other fragility fractures, the incidence of distal tibia fractures did not increase significantly with advancing age (Table 41.1).
CLASSIFICATION
Fractures of the distal tibia and fibula are characterized using two main classification systems. The Rüedi and Allgöwer system, first published in 1968 in German4 but subsequently translated and published in English in 1969,5 is a relatively simple descriptive classification system that divides intra-articular fractures of the distal tibia into three types. Non-displaced intra-articular fractures are classified as type I fractures. Type II fractures involve displacement of the distal tibial articular surface without significant comminution. Type III fractures are displaced intra-articular fractures with significant comminution, often involving articular impaction.
The AO/OTA classification system divides fractures of the distal tibia into three main types: extra-articular (type a), partial articular (type b) and complete articular (type c) as depicted in Figure 41.1.6 Fractures in each type are then classified on the basis of fracture comminution into one of three groups, each of which can be further subdivided into three subgroups based upon other fracture characteristics. With its 27 resultant fracture types, the AO/OTA classification system is a comprehensive descriptive system designed to include all possible fractures of the distal tibia, both extra-articular and intra-articular.
While Martin et al.7 demonstrated better interobserver reliability with the AO/OTA classification system (kappa = 0.60) than with the Rüedi and Allgöwer system (kappa = 0.46), Swiontkowski et al.8 showed that the interobserver reliability of the AO/OTA classification system was highest for determining fracture type (A, B or C, kappa = 0.57) and lower for fracture group (kappa = 0.43) and subgroup (kappa = 0.41). Despite only achieving moderate overall interobserver reliability scores, both of these systems can be useful clinically (for effective communication among healthcare workers, determining an appropriate treatment plan and preoperative planning) and for research purposes.
Table 41.1 Distal tibia fracture incidence per 100,000 population in individuals aged 65 and above, grouped in 5-year age ranges, with P values calculated between groups
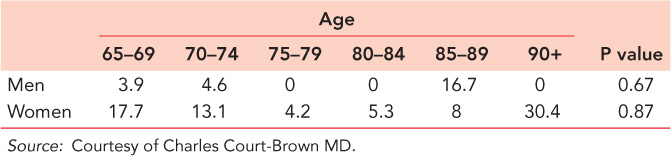
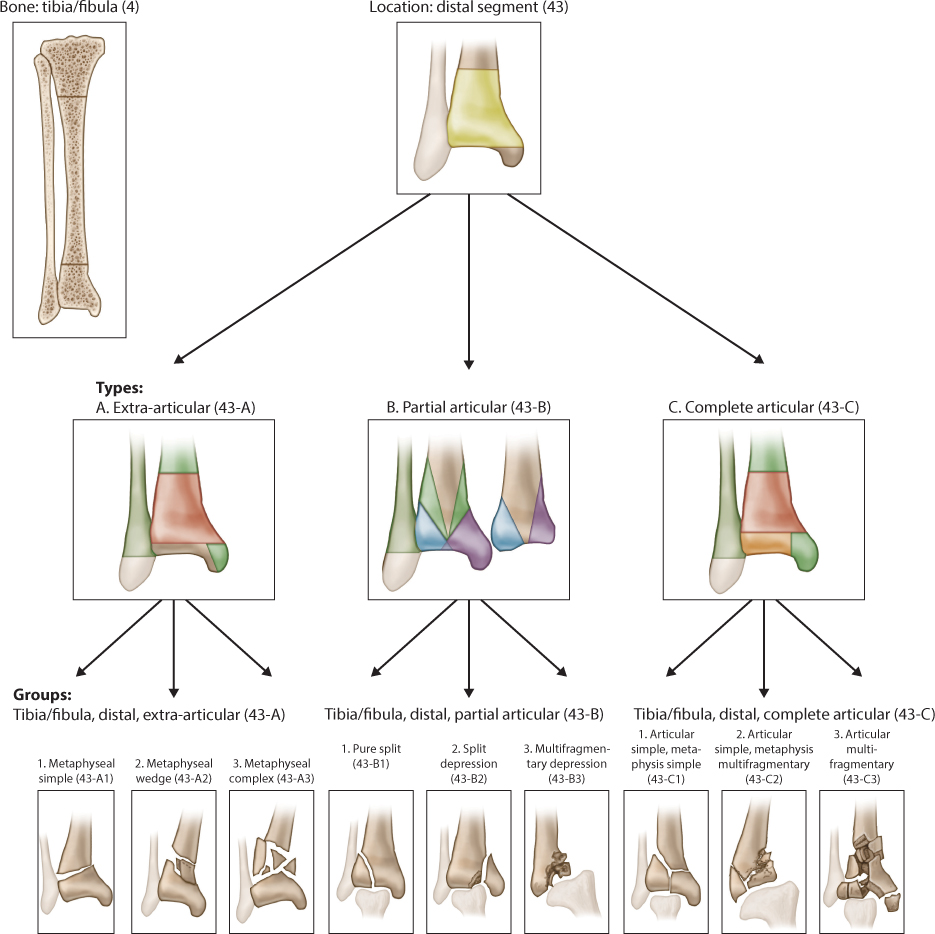
Figure 41.1 AO/OTA Classification System for Distal Tibia and Fibula Fractures. (Reproduced with permission from Marsh JL et al. J Orthop Trauma. 2007; 21(10 Suppl): S1–133.)
TREATMENT
Multiple treatment options exist for fractures of the distal tibia in the elderly. Radiographs of the entire tibia and ankle are required for a complete assessment of the fracture pattern and bone quality. A key determination to make is whether the fracture is extra-articular or intra-articular. If intra-articular extension is present or suspected, advanced imaging with computed tomography may assist in further characterization of the fracture, including any articular incongruity, impaction or comminution.
Although the majority of distal tibia fractures in the elderly occur as the result of low-energy mechanisms of injury, a careful assessment of the soft tissue envelope is essential. The degree of soft tissue injury, presence of open wounds or chronic venous stasis, baseline cellulitis and location of any previous surgical scars must be noted when considering both operative and non-operative treatment options. Likewise, patient comorbidities (such as diabetes, cardiovascular disease and peripheral vascular disease) and risk factors for wound complications (such as smoking, poor nutrition and immunosuppression) must be identified and optimized prior to any proposed surgical intervention. Finally, a patient’s functional demands, including ambulatory status, level of independence and support system must be considered in the development of an individualized treatment plan.
Non-operative treatment
Non-operative treatment was used almost exclusively for treatment of extra-articular fractures of the distal tibia through the 1960s. Although evidence based guidelines for tibial alignment do not exist, acceptable criteria for non-operative management have included fracture shortening of less than 1 cm, less than 5 degrees of valgus and 0 degrees of varus, less than 10 degrees of angulation in the sagittal plane and 5–10 degrees of external rotation and no internal rotation.9 In a series of more than 700 tibial shaft fractures which included proximal, mid-shaft and distal fractures, Nicoll reported a malunion rate of only 8.6%.10 However, Coles and Gross reported a 31.7% rate of malunion, a 13.1% rate of delayed union and a 4.1% rate of non-union in their systematic review of the prospective literature, which identified 145 tibial fractures treated non-operatively.11 High rates of associated ankle and knee stiffness (25% in Nicoll’s series) have also been reported with non-operative treatment.
Sarmiento popularized the functional brace for the closed treatment of proximal, diaphyseal and distal tibia fractures. In a large case series of 450 distal tibia fractures treated with the functional brace, Sarmiento and Latta reported a non-union rate of only 0.9%.12 Less than 10% of patients had an angular deformity greater than 6 degrees in any plane, and varus deformity was more commonly seen in the setting of an intact fibula. Two-thirds of patients healed with less than 5 degrees of deformity in any plane, and 90% healed with a deformity of less than 8 degrees. An average of 5.1 mm of shortening was reported, and 94.2% of patients healed with less than 12 mm of shortening. Mean fracture shortening did not change from injury to fracture union, leading the authors to conclude that axially unstable distal tibia fractures do not undergo further shortening when treated non-operatively in a functional brace. These favorable results are comparable to the results achieved in Sarmiento’s even larger case series of over 1000 closed diaphyseal tibia fractures treated with the functional brace, with union occurring in over 99%.13
Non-operative management of intra-articular fractures of the distal tibia has proven to be less successful. In a small case series of 19 pilon fractures, Ayeni reported good clinical outcomes in 11 Rüedi and Allgöwer type I fractures treated non-operatively but universally poor clinical outcomes in the three type II fractures treated non-operatively.14 Kellam and Waddell classified 26 pilon fractures into two groups based on fracture pattern (rotational versus compressive).15 For both groups, clinical results after non-operative treatment were inferior to those obtained with surgical treatment, and non-operative treatment was only successful in rotational injuries that did not displace over the course of treatment. Based on these and other case series, non-operative treatment is best reserved for non-displaced intra-articular distal tibia fractures that are unlikely to displace during cast immobilization. In addition, non-operative management may still be the preferred method of treatment for certain elderly patients with intra-articular distal tibia fractures. Non-ambulatory patients (including those with quadriplegia or paraplegia), patients with absolute contraindications to surgical treatment (critical aortic stenosis or other unstable cardiopulmonary conditions) and those with limited functional capacity (dementia/Alzheimer) or metabolic bone diseases such as osteogenesis imperfecta may be best served with non-surgical treatment (Figure 41.2).
External fixation
External fixation is a useful technique for provisional fixation of distal tibia fractures in the setting of significant open wounds or severe soft tissue swelling. Multiple techniques of external fixation can be utilized including thin-wire, half-pin and hybrid constructs (combining thin wires and half pins). Although anatomically ‘safe corridors’ have been described for thin-wire fixation in the distal tibia, a cadaveric study in which surgeons familiar with such corridors each placed two thin wires in the distal tibia demonstrated that 55% of wires impaled at least one tendon that crossed the ankle joint.16 Other structures at risk with thin wire fixation were the saphenous vein, superficial peroneal nerve and superior capsular reflection of the ankle joint, which extended an average of 32 mm above the medial malleolus and 21 mm above the anteromedial joint line.
External fixation is generally less successful than other methods of fixation in the definitive treatment of distal tibia fractures. In a prospective comparative trial at multiple level 1 trauma centers, Richards et al. assessed outcomes after fixation of intra-articular distal tibia fractures treated by delayed open reduction internal fixation (ORIF) versus definitive external fixation.17 External fixation was associated with a significantly higher rate of delayed union or non-union (22.2% vs 3.7%, P = 0.05), and the ORIF group had significantly better Short Form-36 (SF-36) physical function scores at 6 months and Iowa Ankle Scores at 6 and 12 months. There were no differences between groups in preoperative patient or fracture characteristics, quality of articular reduction or rates of deep infection.
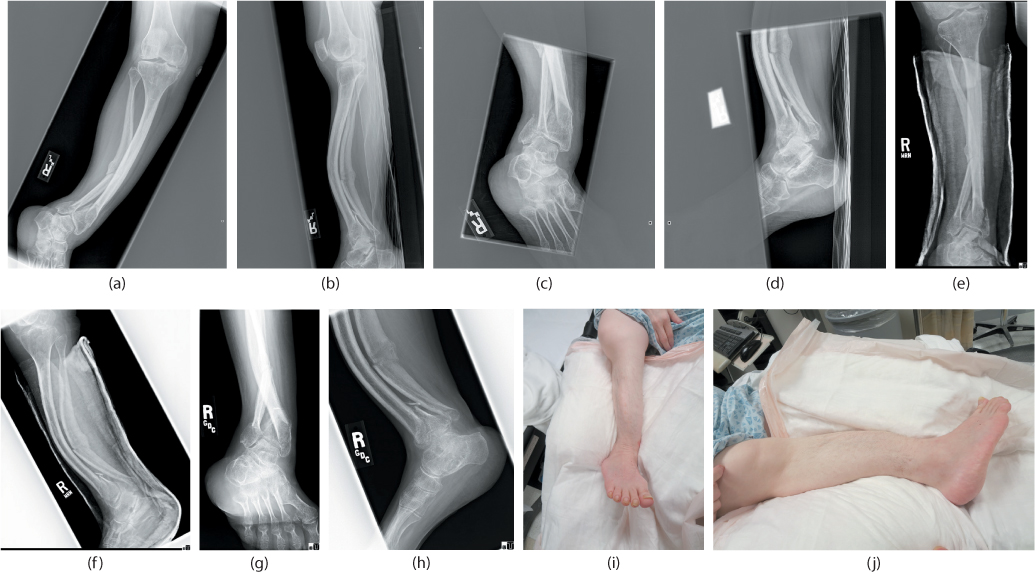
Figure 41.2 A 55-year-old woman with osteogenesis imperfecta sustained an extra-articular right distal tibia fracture in a motor vehicle collision. Anteroposterior (AP) and lateral views of the tibia (a,b) and ankle (c,d) are shown. Based on the patient’s non-ambulatory status and poor bone quality, non-operative management was chosen and a short-leg splint was applied (e,f). X-rays at 16 weeks after injury showed abundant callus formation and healing (g,h). The patient was able to return to her baseline level of function, using the right lower extremity for transfers. Clinical photos (i,j) demonstrate alignment satisfactory for her required level of mobility.
Plate fixation
In the 1970s, plate fixation began to supplant non-operative treatment as the preferred method of managing distal tibia fractures. Multiple anatomic locations in the distal tibia are amenable to plate fixation. Lee et al. retrospectively reviewed 88 patients with distal tibia fractures treated with an anterolateral plate (n = 49) or a medial plate (n = 39).18 The authors found no difference in rates of operative time, fracture union, malunion, ankle range of motion or functional outcomes, but medial plating was associated with a higher rate of hardware complications and total complications.
Concerns for wound infection and hardware prominence have led to the development of techniques for plate insertion that both minimize disruption of the fracture environment and limit the extent of additional injury to the often tenuous soft tissue envelope of the distal tibia. Minimally invasive plate osteosynthesis (MIPO) involves making relatively small periarticular incisions through which the distal-most aspect of the plate is positioned appropriately on the bone. Submuscular (extraperiosteal) dissection is then performed with relatively atraumatic instruments in order to ‘slide’ the plate proximally. Proximal holes in the plate are filled in a percutaneous manner with stab incisions and often a counter-incision over the proximal end of the plate. Bloomstein et al. have described a helpful technique for percutaneous plate application.19 Using a suture tied to the proximal portion of the plate enables manipulation of both poles of the plate, which assists in achieving anatomic plate positioning while simultaneously avoiding soft tissue stripping. The MIPO technique can be utilized in a variety of clinical scenarios in which the soft tissue envelope is at risk.
Collinge et al. evaluated clinical outcomes in 26 high-energy distal tibia fractures with minimal or no intra-articular extension treated with minimally invasive medial plating.20 There were two cases of loss of fixation (8%), and all but one case achieved acceptable alignment, defined as shortening <1 cm and angulation <5 degrees in any plane. Risk factors for healing problems included significant fracture comminution, bone loss and high-grade open fractures, and 35% of patients required secondary procedures to achieve union. Nonetheless, SF-36 functional outcomes scores had returned to normal in 81% of patients at 2 years.
More recently, Collinge and Protzman reported functional outcomes in 38 patients with distal tibia fractures treated with a hybrid MIPO technique (using locking and non-locking screws above and below the fracture).21 Fracture union was achieved in all cases, malalignment and loss of fixation each occurred in one patient (3%), and two patients (6%) required secondary procedures to achieve union. Good to excellent functional outcomes on the American Orthopaedic Foot and Ankle Surgeons’ (AOFAS) and Olerud and Molander scales were attained by 30 of 38 patients (79%), and mean SF-36 scores were only significantly diminished in the physical function domain when compared to normative data. In a similar study, Oh et al. reported 100% union in 21 distal tibia fractures treated with MIPO.22 There were no cases of sagittal or coronal malalignment >5 degrees, and only one case of malrotation (10 degrees of internal rotation) occurred. Outcomes in elderly distal tibia fractures treated with MIPO are more likely to approximate those of the latter two studies, which represented a spectrum of low and high-energy injuries with an age range of 17–82 years.
As MIPO has gained popularity, some concern has arisen regarding injury to neurovascular structures at risk with the various surgical approaches to the distal tibia. Wolinsky and Lee performed a cadaveric study to investigate the relationships between an anterolateral distal tibia plate and important neurovascular structures in the lower leg.23 Using a pre-contoured anterolateral plate designed for minimally invasive submuscular application and percutaneous proximal fixation, the authors identified the superficial peroneal nerve in all 10 cadaveric specimens in the distal wound and concluded that this structure is not at risk. The neurovascular pedicle consisting of the deep peroneal nerve along with the anterior tibial artery and vein lies posterior to the plate proximally but courses anteriorly, crossing over the plate in a consistent region 4–11 cm proximal to the ankle joint, placing them at risk in this location.
In a similar study, Ozsoy et al. investigated the anatomic structures at risk when performing MIPO medially.24 The saphenous nerve and great saphenous vein were most at risk over holes 4, 5 and 6 of the Synthes 3.5/4.5 mm locking compression distal tibial metaphyseal plate and over holes 3, 5 and 8 of the Synthes 3.5 mm locking compression medial distal tibial plate with tab. In order to minimize injury to these neurovascular structures, the authors recommended using careful dissection down to the plate, atraumatic placement of drill sleeves and protection of the soft tissues during screw insertion. Mirza et al. also investigated the risk of injury to the saphenous nerve and vein with the medial MIPO technique.25 Percutaneous placement of smooth Kirschner wires (K-wires) in each hole of the plate caused injury to both structures in every specimen in a reproducible region 2.0–4.7 cm proximal to the tip of the medial malleolus. This study also assessed risk of injury to the superficial peroneal nerve with percutaneous lateral plating of the fibula. The nerve, which was found to exit the lateral compartment fascia an average of 11.5 cm proximal to the tip of the lateral malleolus, was injured in only one of 10 specimens.
Soft tissue considerations such as open wounds, previous scars, extensive swelling or fractures blisters often preclude one or more anatomic approaches to the distal tibia. In such settings, the surgeon must be familiar with multiple surgical approaches and options for fixation. Sheerin et al. reported a technique for fixation of distal tibia fractures with significant anteromedial soft tissue compromise.26 Using a 90-degree cannulated blade plate applied through a posterolateral approach, the authors achieved primary union in 14 of 15 cases; in one case of delayed union, the fracture healed after compression plating with bone grafting. Another useful technique for fixation of distal tibia and fibula fractures in the setting of severe anteromedial soft tissue injury is trans-syndesmotic fixation through the fibula, as described by Sciadini et al.27 In this technique, a 3.5 mm locking compression plate is placed on the posterolateral surface of the fibula after fracture reduction has been performed. Fixation is then extended into the tibia by means of long trans-syndesmotic screws placed through the plate and the fibula (Figure 41.3). Having already passed through two fibular cortices, these screws function as angular stable screws, and together the fibula and plate act as a bridge plate construct for the distal tibia fracture. The authors reported good results with this technique in six patients with minimum follow-up of 14 months (Figure 41.3).
Intramedullary nail fixation
Nork et al. reported excellent outcomes following intramedullary nailing of 36 distal tibia fractures (located within 5 cm of the ankle joint) using two or three distal interlocking screws.28 Acceptable radiographic alignment (<5 degree angulation in any plane) was achieved and maintained in 92% of fractures, and union occurred in all 30 patients who completed follow-up, although three patients (10%) required a staged autograft procedure due to significant traumatic bone loss. Functional outcome scores at 2 years were available for 35% of patients, and SF-36 functional outcomes scores did not differ from normative values in seven of the eight subsets (physical function remained decreased) of this tool. Average Musculoskeletal Function Assessment (MFA) scores at 2 years were better than previously published average MFA scores following isolated knee, leg or ankle injuries. Wysocki et al.29 achieved acceptable alignment (<5 degrees in any plane, <1 cm shortening) in 25 of 27 distal tibia fractures treated with an intramedullary nail by using a two-pin external fixator (‘travelling traction’) during nail passage and locking. Alternatively, a femoral distractor can be used for this same purpose.
Obremskey and Medina investigated rates of malalignment in distal third tibia fractures treated with intramedullary nailing by community orthopaedic surgeons versus orthopaedic trauma specialists.30 Angular malalignment of more than 5 degrees occurred in 23% of fractures treated by community orthopaedic surgeons compared with only 5% of fractures treated by orthopaedic trauma surgeons (P < 0.05). Patients with malaligned fractures had significantly higher bodily pain scores on the Musculoskeletal Outcomes Data Evaluation and Management System (MODEMS) scale than patients with well-aligned fractures. The MODEMS program was launched in the late 1990s by the American Academy of Orthopaedic Surgeons in order to develop standardized assessment criteria and measurement instruments related to the musculoskeletal system. Although the program achieved early success, it never garnered the critical mass of subscribers necessary to become economically viable and financially successful. However, the efforts of the MODEMS program helped set standards for quality in clinical outcomes research on the musculoskeletal system.

Figure 41.3 Preoperative anteroposterior (AP) and lateral X-rays (a,b) of an elderly woman who sustained a type IIIa open distal tibia and fibula fracture with a large medial wound. Trans-syndesmotic fibular plating was carried out through a posterolateral approach to provide fixation of both fractures through a favourable soft tissue envelope (c,d). AP and lateral X-rays 6 months after fixation (e,f) show healing of the fractures with excellent alignment. Uncomplicated healing of the medial traumatic wound and the posterolateral surgical incision were achieved (g,h). (Courtesy of Marcus Sciadini MD.)
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


