Total Knee Arthroplasty—Varus Deformity: Medial Release
Varus deformity is the most common deformity encountered in osteoarthritis of the knee. Bone loss from the posteromedial aspect of the tibial plateau may be encountered, along with contracture of the medial capsule, deep medial collateral ligament (MCL), pes anserine tendon insertions, pos-teromedial corner, and semimembranosus and superficial MCL. Historically, release of the contracted soft tissues on the medial aspect of the knee has allowed for adequate correction of alignment and satisfactory clinical results.1,2
Diagnostic Tests
- Standard radiographs: weight-bearing anteroposterior (AP) and 45-degree flexion posteroanterior (PA) views, and Merchant and lateral views.
- Full-length standing AP radiograph of the entire limb.
Preoperative Planning and Timing of Surgery
- Physical examination should determine the degree of deformity, range of motion, and muscle strength of the knee.
- Evaluation of mechanical axis of the ipsilateral limb and degree of deformity from a standing three-joint view
- Determination of the angle between the mechanical and anatomic axes of the ipsilateral femur for determining valgus angle of the distal femoral resection
- Ideal postoperative alignment is independent of the original anatomy and should not be compared with that of the opposite, “normal” knee, because it most likely has a similar angular deformity.
- The objective in correcting a fixed angular deformity of the knee is to restore the mechanical axis of the extremity to 0 degrees.
- Bone loss from the posteromedial aspect of the tibial plateau is not uncommon and should be assessed for the possibility of bone grafting or modular metallic augments.
Anesthesia
Epidural anesthesia with intravenous sedation as needed and postoperative epidural patient-controlled analgesia (PCA); or general anesthesia with postoperative intravenous (IV) PCA
Patient Position
Supine on regular operative table
Surgical Procedure
- Anterior, midline skin incision beginning about 6 to 8 cm proximal to the superior pole of the patella and extending the same distance distal to the inferior pole.
- Distal incision should run just medial to the medial edge of the tibial tubercle rather than over the prominence.
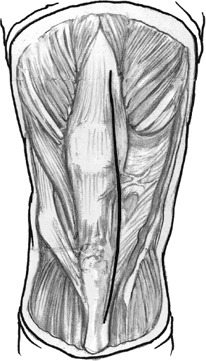
- Medial arthrotomy, beginning at the apex of the quadriceps tendon running distally leaving approximately 1/2-cm cuff of tendon on the medial border. Arthrotomy is continued over the medial border of the patella and extends distally just medial to the medial border of the patellar tendon (Fig. 34–1).
- The quadriceps expansion is peeled from the anterior surface of the patella by sharp dissection until the medial border of the patella is visualized.
- Soft tissue and ligamentous release is performed prior to bone cuts.
- Ligamentous balance is achieved by progressively releasing the tight medial soft tissues until they reach the length of the lateral ligamentous structures.
- With the knee in extension, a subperiosteal sleeve is elevated sharply from the proximal medial tibia including the medial capsule, deep MCL, and insertion of the pes anserinus tendons (Fig. 34–2).
- Placement of a Homan retractor allows traction on the medial soft tissues, facilitating the subperiosteal release.
- The capsular sleeve is dissected subperiosteally with an elevator beyond the midcoronal plane to the level of the posteromedial corner of the knee joint, and the insertion of semimembranosus is released (Fig. 34–3).
- The distal attachment of the superficial MCL can be left intact initially.
- A straight 3/4-inch osteotome is used to elevate the distal insertion of the superficial MCL (Fig. 34–4).
- The extent of the release is monitored by periodically inserting lamina spreaders into the tibiofemoral joint and judging limb alignment with the aligning rod or plumb line. The end point of the release is a stable knee in which the plumb line extends through the centers of the hip, knee, and ankle (Fig. 34–5).
- If the posterior cruciate ligament (PCL) is tethering the release, it should be excised or lengthened by a posterior release from the tibia.
- Knee flexed and tibia externally rotated facilitating exposure of the posteromedial corner and release of the insertion of semimembranosus and posterior capsule
- Excise osteophytes from the medial aspect of the distal femur and proximal tibia, including the protruding flare of the tibial plateau.
- Posteriorly, the release may include the deep fascia investing the soleus and popliteus muscles.
- When the medial release is complete and the limb is aligned in the proper position, the bone cuts can be made in the standard manner.
- Posteriorly, the release may include the deep fascia investing the soleus and popliteus muscles.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


