2 The Subvastus Approach
Patient Presentation and Symptoms
The subvastus approach is an alternative approach for total knee arthroplasty. While often discussed in the previous decade, it has had resurgence because of the minimally invasive surgery techniques recently described. This approach is an alternative to performing a total knee arthroplasty.
Indications
This approach is indicated for patients undergoing total knee arthroplasty with the subvastus approach and alternative approach. Large obese limbs as well as very muscular limbs may be difficult to operate on with a subvas-tus approach. A standard medial arthrotomy may need to be required in these cases.
Contraindications
Contraindications include severe patellar baja, previous medial arthrotomy with scarring, large obese extremity, and large muscular limb.
Special Considerations
Intraoperative evaluation of the patellofemoral joint can be performed. The medial flap can be created and the vastus medialis oblique (VMO) mobility assessed prior to starting medial arthrotomy or the subvastus approach.
Special Instruments
Adequate retractors are needed, especially if the minimally invasive approach is utilized. Ninety-degree right-angle retractors, bent Hohmann retractors, and Bennett retractors are helpful in providing adequate exposure.
Anesthesia
Standard anesthesia techniques are applicable. No special anesthesia protocol is required for the subvastus approach.
Patient Position
The patient is placed in the supine position.
Surgical Procedure
The subvastus approach is performed in four main steps:
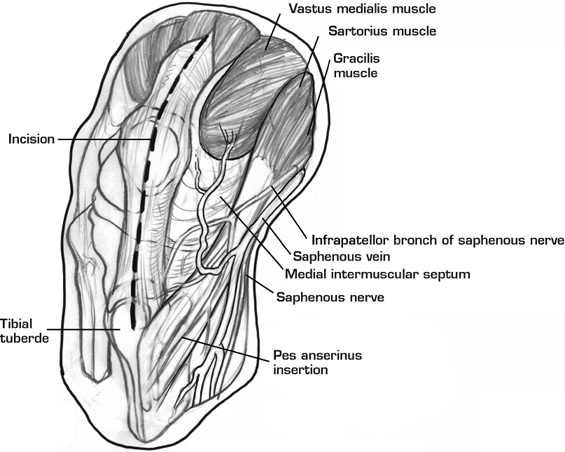
- A midline incision is made through the skin and superficial fascia from the level of the superior edge of the quadriceps tendon proximally to the level of the tibial tubercle distally (Fig. 2–1).
- The vastus medialis is bluntly dissected and elevated away from the medial intermuscular septum (Fig. 2–2). This step must be performed very carefully as greater than 10 cm proximal dissection can injure the intermuscular septal branch or the articular branch of the descending genicular artery.
- An incision is made transversely through the medial retinaculum, inferior to the vastus medialis from the medial side. When the patellar tendon is reached, the incision is stopped and a new one is made in the sagittal plane just medial to the patellar tendon to the level of the tibial tuberosity (Fig. 2–3).
- The patella and extensor mechanism can be everted and the knee can be exposed in flexion. Certainly much of the exposure and patellar preparation can be performed with lateral displacement of the patella rather than complete eversion.
Dressings, Braces, Splints, and Casts
Standard postoperative dressings are utilized.
Tips and Pearls
Rather than severing the insertion of the vastus medialis from the quadriceps tendon and medial parapatellar retinaculum, as in the paramedian approach, the subvastus approach preserves the extensor mechanism by elevating the inferior border of the vastus medialis from the medial intermuscular septum and adductor aponeuro-sis (Fig. 2–4). Furthermore, not severing the vastus medialis from the quadriceps tendon also allows for the blood supply from the descending genicular artery and its branch to be preserved.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


