Arthroscopic Lateral Retinacular Release
Patient Presentation and Symptoms
- Lateral patellar dislocation
- Patellar catching or giving way
- Anteromedial knee pain
Indications
Malalignment with recurrent subluxation or dislocation of the patella that has been refractory to nonoperative management
Physical Examination
- Apprehension
- Medial retinacular tenderness
- Abnormal patellar tracking through a range of motion
Patient and Equipment Positions
- Supine on the operating table
- No leg holder
- Thigh tourniquet applied but not inflated
Surgical Procedure
Surgical Approach
Arthroscopic Portals
- Superomedial inflow portal
- Inferolateral arthroscopy portal
- Inferomedial portal
Surgical Technique
- Arthroscopic examination through the inferolateral portal, paying close attention to patellofemoral tracking, lateral facet compression, and chondromalacia
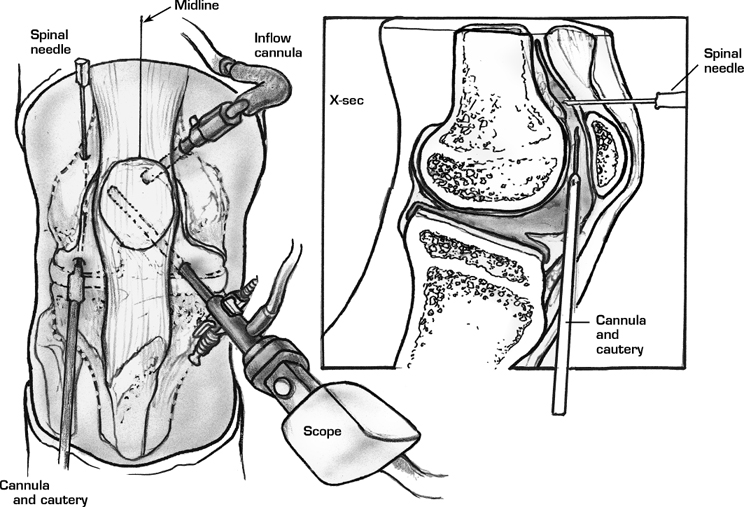
- Transfer the arthroscope to the inferomedial portal (Fig. 49–1)
- Insert a spinal needle approximately 2 cm proximal to the superolateral margin of the patella. This helps in orientation during the release.
- Insert the arthroscopic electrocautery unit or ultrasound wand through the inferolateral portal.
- Begin the lateral release at the musculotendinous junction of the vastus lateralis near the superolateral border of the patella.
- Transect the synovium and capsular ligaments sequentially (Fig. 49–2).
- Progress with the release distally, staying approximately 1 cm from the patella.
- Adequate release is confirmed by manually everting the patella 90 degrees.
Dressings, Braces, Splints, and Casts
Standard postoperative dressings including an Ace bandage
Postoperative Care
- Immediate range of motion exercises
- Weight bearing as tolerated, initially with crutches
- Reestablish the dynamic equilibrium between the hamstrings and quadriceps.
Tips and Pearls
- Maintain the layer of subcutaneous fat as this layer acts as an insulator against cutaneous burns from the cautery unit.
- To ensure an adequate release, the lateral patellotibial ligament and capsular tissue must be released.
- The inferolateral arthroscopy portal may be enlarged as a small arthrotomy to complete the distal release.
Related posts:
 Knee Replacement: The Midvastus Approach
Open Reduction and Internal Fixation of Intra-articular Distal Femur Fractures
Meniscus Repair: Outside-In Technique
Ligament Advancement in Total Knee Arthroplasty
Chondral Injuries Treated with Osteochondral Autograft Transfer
Rupture of the Patellar Tendon
Knee Replacement: The Midvastus Approach
Open Reduction and Internal Fixation of Intra-articular Distal Femur Fractures
Meniscus Repair: Outside-In Technique
Ligament Advancement in Total Knee Arthroplasty
Chondral Injuries Treated with Osteochondral Autograft Transfer
Rupture of the Patellar Tendon
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


