Total Knee Arthroplasty: Posterior Cruciate Ligament Recession
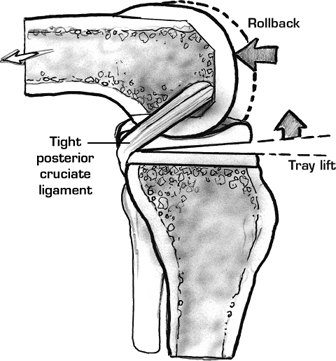
Preservation of the posterior cruciate ligament (PCL) in total knee arthroplasty (TKA) has been advocated to reproduce more normal knee kinematics, preserve anatomic femoral rollback, preserve anterior femoral–tibial contact in extension, and increase range of motion.1 However, for the PCL to function properly, it must be tensioned appropriately, and not be left too loose or more commonly too tight.2 A tight PCL can cause excessive femoral rollback, impingement of the tibial polyethylene insert posteriorly with subsequent polyethylene wear and debris formation, and limited knee flexion (Fig. 37–1). In addition, more conforming tibial inserts that provide more contact area and less contact stresses require a balanced PCL to prevent a kinematic conflict with femoral rollback. Therefore, at the time of PCL-retaining TKA, a partial release or recession of the PCL may be required to balance this important structure and obtain the best outcome possible for the arthroplasty.3
Indications
Total knee arthroplasty with a PCL-retaining prosthesis, where the PCL is found to be tight after all appropriate bone cuts are made and the trials have been inserted
Contraindications
- In patients where the ligament cannot be recessed sufficiently to balance it, a PCL substituting prosthesis should be used.
- In patients with a flexion contracture over 20 degrees and a varus or valgus deformity over 15 degrees, it becomes extremely difficult to balance the PCL, and consideration should be given to using a PCL substituting prosthesis.
Physical Examination
In the examination of the arthritic knee preoperatively, the PCL is almost always intact and functioning, unless there has been a previous injury. One is not able to discern clinically if the ligament is excessively tight and whether it will require release.
Diagnostic Tests
Radiographs of the involved knee, including standing anteroposterior, standing tunnel, lateral and sunrise views
Special Considerations
One must be careful to obtain a knee with equal flexion and extension gaps after the bone cuts are made and all ligaments are balanced. A tight flexion gap must be carefully evaluated under direct visualization during surgery with the use of unconstrained tibial trials. If the trial tibial insert, or the tibial tray itself, lifts off anteriorly from the tibial bone during flexion, then a tight flexion gap exists and must be balanced (Fig. 37–2). Before resorting to further bone cuts, the surgeon should examine the PCL and perform a recession if it is found to be tight.
Preoperative Planning and Timing of Surgery
When patients have disabling knee pain with limitations in their daily activities, their quality of life is compromised. Radiographs demonstrate—and templating should be performed to determine—the relative amounts of bone to be removed, the amount of soft tissue releasing and balancing that may be required, and the approximate size of components to be used.
Special Instruments
- Electrocautery
- PCL retractor to sublux the tibia forward and expose the PCL insertion down the posterior aspect of the tibia
- Periosteal elevator
Anesthesia
Although general or regional anesthesia can be used for TKA, our preference is a regional anesthetic, specifically spinal analgesia with Duramorph.
Patient and Equipment Positions
The patient is placed supine on the operating table, with a small bump under the ipsilateral buttock and a fixed bump near the end of the bed that allows the knee to remain flexed at 90 degrees with the foot placed up against it.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


