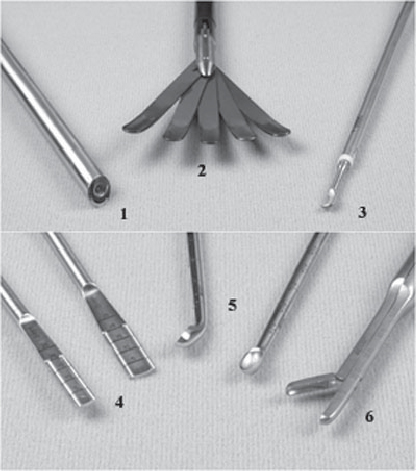
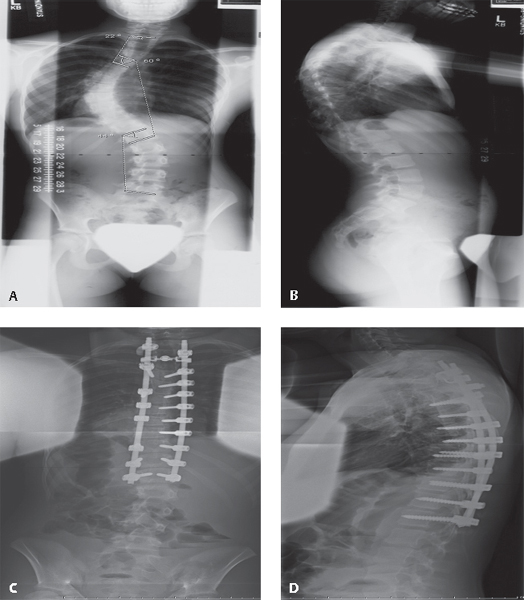
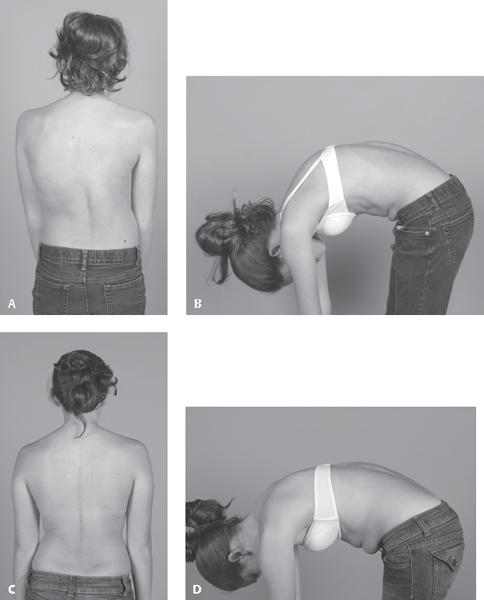
57 Thoracoscopy is the endoscopic technique of gaining access to the intrathoracic cavity using small (~ 1–2 cm) incisions to enable surgical procedures on structures within the chest. Although thoracoscopy was first utilized in the treatment of lung conditions, applications for treatment of the spine have become common and effective.1 Visualization of the structures within the chest is accomplished using a fiberoptic camera. This thoracoscope is usually 10 mm in diameter, has a 30- or 45-degree angled lens, and is long enough to reach significant depths within the chest, thus providing the surgeon the ability to look around corners and allowing improved visualization as compared with open techniques. The remaining working portals allow for long rongeurs, electrocautery, curettes, osteotomes, suction devices, and suturing instruments to be placed into the chest (Fig. 57.1). These instruments allow the surgeon to perform many types of surgical procedures for anterior thoracic spinal pathology. The goal of the thoracoscopic approach is to provide excellent visualization and the ability to duplicate the safety and efficacy of performing anterior thoracic surgery achieved through an open thoracotomy approach.2,3 The indications for thoracoscopy in the treatment of spinal conditions are essentially the same as those for an open thoracotomy approach. Candidates for thoracoscopy include patients with severe spine deformity requiring anterior release, skeletally immature patients requiring anterior fusion to avoid the crankshaft phenomenon, and patients requiring anterior instrumentation and fusion (Fig. 57.2A–D and Fig. 57.3A–D).4 Thoracoscopy can be used in the setting of spinal infection or vertebral column or spinal cord tumors to obtain cultures/biopsy or for débridement/resection and placement of anterior structural support. Often these anterior surgeries can be supplemented with a posterior approach.5–7 Thoracoscopy can also be used to treat herniated thoracic disks and spine trauma such as burst or compression fractures.8 Pathology can be treated from T1 to L1 using thoracoscopic techniques. Fig. 57.1 Thoracoscopic working instruments. (1) 30 degree thoracoscope, (2) fan retractor, (3) ultrasonic harmonic scalpel hook blade, (4) disk shavers, (5) curettes, (6) rongeur. Contraindications to thoracoscopy include patients with significant respiratory problems, since single-lung ventilation is required when performing thoracoscopy in the lateral position. Patients who have had previous anterior surgery with significant intrathoracic adhesions and scarring make entrance into the chest difficult; thus, previous thoracic surgery is a relative contraindication for thoracoscopy. Compared with an open thoracotomy approach, there are several advantages to thoracoscopy that are related to the smaller incisions and less chest wall injury (Table 57.1). The main disadvantage of thoracoscopy in the treatment of spinal conditions is that it is technically demanding and requires advanced training with hands-on courses.9 In addition, thoracoscopy requires single-lung ventilation when performed in the traditional lateral position and may result in significant respiratory complications. This can be avoided by placing patients in the prone position. In this alternative position, double-lung ventilation is achieved with a regular endotracheal tube; however, the anesthesiologist must decrease the tidal volumes by 50–60% and increase respiratory rates to maintain oxygen saturation.10 The intraoperative cost of thoracoscopy is greater than that of the traditional thoracotomy approach because of the use of disposable items. Fig. 57.2 Radiographs of a 12+5-year old female (with previously decompressed syringomyelia) who underwent a thoracoscopic anterior spinal release and posterior instrumentation. (A) Preoperative posteroanterior (PA) radiograph demonstrating a 60-degree left thoracic curve with compensatory upper thoracic and lumbar curves. (B) Lateral radiograph demonstrating an upper thoracic kyphosis. (C,D) The postoperative PA and lateral radiographs demonstrating excellent coronal and sagittal plane correction. Positioning of the patient is either in the lateral decubitus position or prone. Single-lung ventilation is necessary in the lateral position and is achieved with a double-lumen endotracheal tube or a Univent tube (Fuji Systems Corp., Tokyo, Japan). This tube allows excellent deflation of the lung; however, it is not well tolerated by some patients. When performing surgery above the T4 or T5 level with the patient positioned laterally, the arm should be included in the surgical field. Access to the T1–T2 level is possible cranially and to the T12–L1 disk distally. The prone position has been described as a good alternative to the lateral position and can achieve similar clinical results with respect to achieving release for spinal deformity, and it has the advantage of significantly less respiratory complications.11 The prone position allows the surgeon to gain excellent access to the spine without requiring single-lung ventilation, and it also allows the surgeon to continue on to the posterior surgery (if planned) without delay. Specially designed instruments are used to manipulate the spine; they are generally modified from standard instruments with longer handles. Endoscopic instruments include a fan retractor, which allows for retraction of the lung; special endoscopic spinal implants for spine deformity and fracture management; and the Endostitch device (U.S. Surgical, Norwalk, CT) for suturing the pleura. Postoperatively, chest tube drainage is necessary for longer, more invasive surgeries and is removed when drainage is decreased (generally to less than 80 mL per shift). Fig. 57.3 Clinical photographs of the patient in Fig. 57.2. (A,B) Preoperative photos (age 12+5) showing sagittal and coronal plane curvature. (C,D) Postoperative photos (age 14+1) showing correction; visible posterior midline, iliac crest harvest, and thoracoscopy scars are well healed. Table 57.1 Advantages and Disadvantages of Thoracoscopy versus Open Thoracotomy
Thoracoscopy
![]() Indications and Contraindications for Thoracoscopy
Indications and Contraindications for Thoracoscopy
![]() Advantages and Disadvantages of Thoracoscopy
Advantages and Disadvantages of Thoracoscopy
![]() Surgical Technique
Surgical Technique
Advantages: |
Smaller incisions, improved cosmesis |
Less chest muscle injury, less postoperative pain |
Less disruption of chest wall mechanics; less detrimental effect on pulmonary function |
Improved intraoperative visualization (camera advances deep into chest) |
Ability to operate on more thoracic levels (simply add more portals) |
Threshold to perform anterior procedure lower (due to above factors) |
Shorter hospital stay |
Disadvantages: |
Technically demanding; need for advanced training |
Single-lung ventilation in lateral position; significant respiratory complications |
Intraoperative cost greater (because of disposable instruments) |
 Thoracoscopy for Trauma
Thoracoscopy for Trauma
There is a body of recent literature that supports conservative management of selected thoracic or lumbar burst fractures. The recently introduced Thoracolumbar Injury Classification and Severity Score (TLICS) defines injury based on three clinical characteristics: injury morphology, integrity of the posterior ligamentous complex, and neurologic status of the patient. On the basis of this classification system, stable burst fractures without neurologic deficit may be treated without surgical intervention.12 However, when surgical intervention is required, thoracoscopic techniques alone or in combination with mini-thoracotomy can be utilized to decompress the spinal cord and reconstruct the vertebral defect.13,14 Fractures from T4 to L2 can be treated using this technique.14 Although technically demanding with a steep learning curve, thoracoscopic treatment offers the advantages of direct visualization of the fracture and better decompression of the canal. Anterior instrumentation, such as plates and cages, can be placed with possibly less radiation exposure than with posterior pedicle screw fixation. Newer reduction plates are available that offer the capability of applying lordotic forces through swivel heads at both ends of the plate. After the plate is fixed to the bridging vertebral bodies, the angulation of the cranial and caudal swivel heads can be changed to provide the appropriate amount of lordosis.14 Finally, thoracoscopic-assisted stabilization of burst fractures may be associated with less postoperative pain and improved restoration of spinal alignment.15,16
References
1. Han PP, Kenny K, Dickman CA. Thoracoscopic approaches to the thoracic spine: experience with 241 surgical procedures. Neurosurgery 2002;51(5, Suppl):S88–S95 PubMed
2. Huntington CF, Murrell WD, Betz RR, Cole BA, Clements DH III, Balsara RK. Comparison of thoracoscopic and open thoracic discectomy in a live ovine model for anterior spinal fusion. Spine 1998;23(15):1699–1702 PubMed
3. Wall EJ, Bylski-Austrow DI, Shelton FS, Crawford AH, Kolata RJ, Baum DS. Endoscopic discectomy increases thoracic spine flexibility as effectively as open discectomy. A mechanical study in a porcine model. Spine 1998;23(1):9–15, discussion 15–16 PubMed
4. Reddi V, Clarke DV Jr, Arlet V. Anterior thoracoscopic instrumentation in adolescent idiopathic scoliosis: a systematic review. Spine 2008;33(18):1986–1994 PubMed
5. Mazel Ch, Grunenwald D, Laudrin P, Marmorat JL. Radical excision in the management of thoracic and cervicothoracic tumors involving the spine: results in a series of 36 cases. Spine 2003;28(8):782–792, discussion 792 PubMed
6. Kan P, Schmidt MH. Minimally invasive thoracoscopic approach for anterior decompression and stabilization of metastatic spine disease. Neurosurg Focus 2008;25(2):E8 PubMed
7. Mückley T, Schütz T, Schmidt MH, Potulski M, Bühren V, Beisse R. The role of thoracoscopic spinal surgery in the management of pyogenic vertebral osteomyelitis. Spine 2004;29(11):E227–E233 PubMed
8. Burke TG, Caputy AJ. Treatment of thoracic disc herniation: evolution toward the minimally invasive thoracoscopic technique. Neurosurg Focus 2000;9(4):e9 PubMed
10. Sucato DJ, Erken YH, Davis S, Gist T, McClung A, Rathjen KE. Prone thoracoscopic release does not adversely affect pulmonary function when added to a posterior spinal fusion for severe spine deformity. Spine 2009;34(8):771–778 PubMed
11. Sucato DJ, Elerson E. A comparison between the prone and lateral position for performing a thoracoscopic anterior release and fusion for pediatric spinal deformity. Spine 2003;28(18):2176–2180 PubMed
12. Patel AA, Vaccaro AR. Thoracolumbar spine trauma classification. J Am Acad Orthop Surg 2010;18(2):63–71 PubMed
13. Kocis J, Wendsche P, Muzík V, Bilik A, Veselý R, Cernohousová I. [Minimally invasive thoracoscopic transdiaphragmatic approach to thoracolumbar junction fractures]. Acta Chir Orthop Traumatol Cech 2009;76(3):232–238 PubMed
14. Schnake KJ, Scholz M, Marx A, Hoffmann R, Kandziora F. Anterior, thoracoscopic-assisted reduction and stabilization of a thoracic burst fracture (T8) in a pregnant woman. Eur Spine J 2011;20(8):1217–1221 PubMed
15. Khoo LT, Beisse R, Potulski M. Thoracoscopic-assisted treatment of thoracic and lumbar fractures: a series of 371 consecutive cases. Neurosurgery 2002;51(5, Suppl):S104–S117 PubMed
16. Ringel F, Stoffel M, Stüer C, Totzek S, Meyer B. Endoscopy-assisted approaches for anterior column reconstruction after pedicle screw fixation of acute traumatic thoracic and lumbar fractures. Neurosurgery 2008;62(5, Suppl 2):ONS445–ONS452, discussion ONS452–ONS453 PubMed
Suggested Readings
Burke TG, Caputy AJ. Treatment of thoracic disc herniation: evolution toward the minimally invasive thoracoscopic technique. Neurosurg Focus 2000;9(4):e9 PubMed
Detailed technique of thoracoscopic discectomy is presented along with the historical progression of treatment methods for thoracic disk herniation.
Han PP, Kenny K, Dickman CA. Thoracoscopic approaches to the thoracic spine: experience with 241 surgical procedures. Neurosurgery 2002;51(5, Suppl):S88–S95 PubMed
This article reports on 241 thoracoscopic procedures. Over all, there was excellent outcome in these patients, and the authors conclude that thoracoscopic techniques can be very effective for many conditions and the complications of an open thoracotomy are avoided.
Huntington CF, Murrell WD, Betz RR, Cole BA, Clements DH III, Balsara RK. Comparison of thoracoscopic and open thoracic discectomy in a live ovine model for anterior spinal fusion. Spine 1998;23(15):1699–1702 PubMed
This animal study compared the open and thoracoscopic anterior thoracic release, demonstrating similar disk removal (76% open vs 68% thoracoscopic), which was not statistically significant. When the disk areas were analyzed with respect to the number in which greater than 50% of the disk was removed, there were 29 of 30 (97%) in the open group, 27 of 30 (90%) in the thoracoscopic approach.
Kan P, Schmidt MH. Minimally invasive thoracoscopic approach for anterior decompression and stabilization of metastatic spine disease. Neurosurg Focus 2008;25(2):E8 PubMed
A small series of five patients treated with thoracoscopic approach for treatment of thoracic and thoracolumbar metastatic spinal cord compression demonstrated improvement in preoperative symptoms and neurologic deficit and no reported complications.
Khoo LT, Beisse R, Potulski M. Thoracoscopic-assisted treatment of thoracic and lumbar fractures: a series of 371 consecutive cases. Neurosurgery 2002;51(5, Suppl):S104–S117 PubMed
This article presents a retrospective review of 371 patients who had a thoracic or thoracolumbar fracture treated with thoracoscopic techniques for fixation of the spine. Anterior surgery alone was done in 35%, with the rest supplemented with posterior surgery. Operative time was long in the early cases but improved with surgeon experience. Complications included one aortic injury, one splenic contusion, one neurologic deterioration, one cerebrospinal fluid (CSF) leak, and one wound infection. A comparison to patients who had treatment with an open technique demonstrated less use of narcotics postoperatively.
Kocis J, Wendsche P, Muzík V, Bilik A, Veselý R, Cernohousová I. [Minimally invasive thoracoscopic transdiaphragmatic approach to thoracolumbar junction fractures]. Acta Chir Orthop Traumatol Cech 2009;76(3):232–238 PubMed
This is a retrospective study of 127 patients with thoracolumbar junction fractures treated with reconstruction of the anterior spinal column via a thoracoscopic procedure with minithoracotomy. Bony fusion occurred within a year of surgery, with average loss of correction of 2 degrees. Improvement of neurologic status by at least one Frankel grade occurred in 10 of the 19 patients with neurologic deficit.
Mazel Ch, Grunenwald D, Laudrin P, Marmorat JL. Radical excision in the management of thoracic and cervicothoracic tumors involving the spine: results in a series of 36 cases. Spine 2003;28(8):782–792, discussion 792 PubMed
The authors describe a combined posterior and thoracoscopic anterior approach to remove tumors en bloc for the small and medium-size thoracic tumors. Thirty-six cases were reported that had the combined technique, with complete vertebrectomy in 7 cases and partial in 29 cases. The authors describe the learning curve but state that selective preoperative screening of patients is essential.
Mückley T, Schütz T, Schmidt MH, Potulski M, Bühren V, Beisse R. The role of thoracoscopic spinal surgery in the management of pyogenic vertebral osteomyelitis. Spine 2004;29(11): E227–E233 PubMed
Three patients who had endoscopic treatment of vertebral osteomyelitis without conversion to an open procedure or posterior procedure. The surgery included radical débridement with anterior reconstruction with good results.
Newton PO, Upasani VV, Lhamby J, Ugrinow VL, Pawelek JB, Bastrom TP. Surgical treatment of main thoracic scoliosis with thoracoscopic anterior instrumentation. Surgical technique. J Bone Joint Surg Am 2009;91(Suppl 2):233–248 PubMed
This article provides a review of surgical technique and examines 5-year results of 25 patients treated at one center with anterior thoracoscopic spinal instrumentation for thoracic scoliosis. Five-year results show that outcomes are comparable with those reported for open anterior and posterior techniques in terms of percent correction of Cobb angle, average total Scoliosis Research Society (SRS) scores, and average total lung capacity as a percent of predicted value. However, there was hardware failure and need for surgical revision in 12% of the patients in this report.
Patel AA, Vaccaro AR. Thoracolumbar spine trauma classification. J Am Acad Orthop Surg 2010; 18(2):63–71 PubMed
This review article discusses the TLICS, which was developed to address the inadequacies of previous classification systems in terms of prognostic information and guiding surgical management. This scoring system defines injury based on three clinical characteristics: injury morphology, integrity of the posterior ligamentous complex, and neurologic status of the patient. The severity score offers prognostic information and is helpful in medical decision making.
Reddi V, Clarke DV Jr, Arlet V. Anterior thoracoscopic instrumentation in adolescent idiopathic scoliosis: a systematic review. Spine 2008;33(18):1986–1994 PubMed
This review of patients with adolescent idiopathic scoliosis treated with anterior thoracoscopic instrumentation compared with open anterior and posterior procedures was based on eight included articles from multiple literature search databases. It concluded that curve correction was similar between techniques, and two studies showed increased patient satisfaction with thoracoscopy, but there was slightly greater operative and ICU time compared to open procedures.
Ringel F, Stoffel M, Stüer C, Totzek S, Meyer B. Endoscopy-assisted approaches for anterior column reconstruction after pedicle screw fixation of acute traumatic thoracic and lumbar fractures. Neurosurgery 2008;62(5, Suppl 2):ONS445–ONS452, discussion ONS452–ONS453 PubMed
This is a prospective study of 83 patients with 100 acute thoracic or lumbar vertebral fractures treated with posterior pedicle screw instrumentation followed by thoracoscopic or endoscopic anterior approach for anterior column reconstruction. Conversion to an open approach was needed in five cases. Complications included: need for repositioning of ventral graft, L1 nerve root injury, posterior wound infection, pleural empyema in one case each, and two cases of transient neurologic worsening.
Schnake KJ, Scholz M, Marx A, Hoffmann R, Kandziora F. Anterior, thoracoscopic-assisted reduction and stabilization of a thoracic burst fracture (T8) in a pregnant woman. Eur Spine J 2011;20(8):1217–1221 PubMed
This is a case report of a pregnant 24-year-old woman whose burst fracture was treated using an anterior thoracoscopic-assisted reduction and stabilization. The body of T8 was removed and a titanium plate was placed from T7 to T9 to stabilize the fracture. Correction of kyphosis was achieved with distraction through the plate. Tricortical iliac bone graft was then press-fitted into the defect.
Sucato DJ. Thoracoscopic anterior instrumentation and fusion for idiopathic scoliosis. J Am Acad Orthop Surg 2003;11(4):221–227 PubMed
This review article discusses thoracoscopically assisted surgery along with indications for this procedure, anesthesia considerations, surgical technique (including instrumentation and correction maneuvers), early results, and complications associated with this technique. It highlights the advantages of improved cosmesis and limitation of chest wall compromise compared to open anterior procedures, and preservation of motion segments compared to posterior surgery. In addition, the article emphasizes that great attention must be paid to proper patient selection, anesthesia considerations, and potential complications.
Sucato DJ, Newton PO, Betz R, et al. Defining the learning curve for performing a thoracoscopic anterior spinal fusion and instrumentation for AIS: A multi-center study. 39th Annual Meeting of the Scoliosis Research Society. Buenos Aires, Argentina, 2004
This retrospective study from 9 institutions evaluated 147 patients, demonstrating a significant improvement in the surgical time and the incidence of complications. A probability analysis demonstrated that surgeons will have a 95% chance of no complications once they have done 35 thoracoscopic anterior instrumentations and fusions.
Sucato DJ, Erken YH, Davis S, Gist T, McClung A, Rathjen KE. Prone thoracoscopic release does not adversely affect pulmonary function when added to a posterior spinal fusion for severe spine deformity. Spine 2009;34(8):771–778 PubMed
This prospective clinical study compared patients who had prone thoracoscopic release with double lung ventilation followed by posterior spinal fusion and instrumentation (PSFI) to patients who had only PSFI for severe idiopathic scoliosis. Excellent coronal correction was achieved without detrimental effect on pulmonary function. Thoracoplasty had a negative effect on pulmonary function.
Sucato DJ, Elerson E. A comparison between the prone and lateral position for performing a thoracoscopic anterior release and fusion for pediatric spinal deformity. Spine 2003;28(18): 2176–2180 PubMed
This retrospective study demonstrated that patients who had a thoracoscopic release followed by a PSFI in the prone position had similar postoperative curve corrections as those who had the anterior release performed in the lateral position. However, because of the same position for the anterior and posterior surgeries with a regular endotracheal tube, the surgical times were less, patients had less postoperative respiratory difficulties, and the need for postoperative oxygen was less.
Wall EJ, Bylski-Austrow DI, Shelton FS, Crawford AH, Kolata RJ, Baum DS. Endoscopic discectomy increases thoracic spine flexibility as effectively as open discectomy. A mechanical study in a porcine model. Spine 1998;23(1):9–15, discussion 15–16 PubMed
This animal model studied the flexibility of the thoracic spine following anterior thoracic discectomy comparing the open and thoracoscopic techniques. There was no difference in the flexibility of the spines when the two techniques were compared.
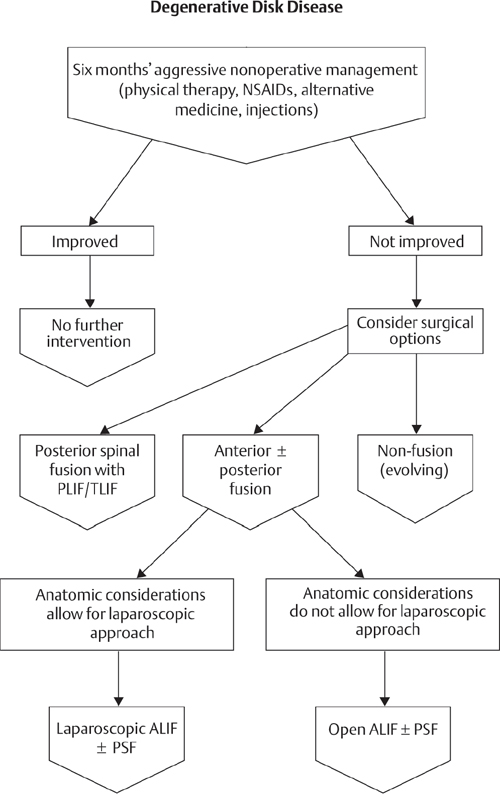
NSAIDs, nonsteroidal anti-inflammatory drugs; PLIF, posterior lumbar interbody fusion; PSF, posterior spinal fusion; TLIF, transforaminal lumbar interbody fusion
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


