Fig. 1
This 45-year-old female presented with groin pain at the right hip. She has got global pincer impingement caused by coxa profunda. The teardrop is located medial to the ilio-ischial line. The center-edge angle is 45°
This chapter describes a surgical reconstruction technique that involves anterior-to-posterior rim trimming followed by a circumferential reconstruction of the labrum with a semitendinosus allograft to restore the labral sealing function.
Surgical Technique
Preop planning. A reconstruction of the labrum is anticipated in case of radiographic signs of generalized impingement in accordance to specific signs for labral stretching such as the recess sign (Fig. 2). On a preoperative x-ray of the pelvis, the lateral center-edge angle of Wiberg is defined [5, 6]. This angle should be ≤39° and a rim trimming is planned with a resection of 1 mm for every degree of over-coverage [7]. The patient should be informed about the potential need for allograft tissue.

Fig. 2
The recess sign is a radiographic indentation sign of the lateral acetabular rim indicating an overgrowth of the labrum by the acetabular bone [1]. This indicates that the labrum is stretched and will be hypoplastic. This labrum probably needs reconstruction after rim trimming
Procedure. The surgical dislocation is performed according to the technique described by Ganz et al. [8]. In brief, the patient is positioned in lateral decubitus. The Gibson approach is conducted and the tip of the greater trochanter is identified in 30° of internal rotation (Fig. 3). The piriformis and gluteus minimus muscles are identified. The trochanteric branch of the medial circumflex artery is identified and a Z-shaped step-cut osteotomy of the trochanter is made. Approximately 3 mm of the tip of the trochanter are left in place. Care is taken to leave the anterior cortex intact in order to fracture the cortex, which will ensure anterior stability when the osteotomized fragment is put back in place. The gluteus minimus muscle is then carefully released from the underlying capsule, which will be incised in a Z-shape to avoid damaging the medial femoral circumflex artery at the level of the femoral neck (Fig. 4). The femoral head is then dislocated out of the acetabulum with an external rotation-flexion maneuver. The ligamentum teres is cut with a curved scissors, which then allows for posterior dislocation of the head beyond the posterior rim. Anterior, superior, and posterior retractor placement provides full visualization of the hip joint and the acetabular rim (Fig. 5).
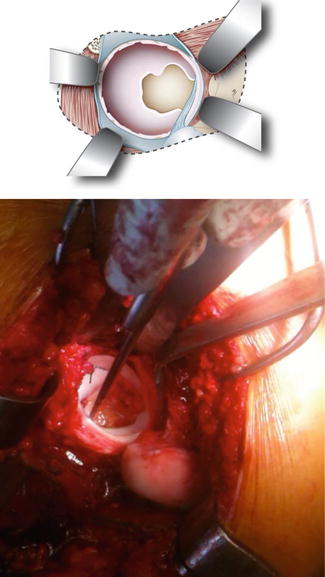
Fig. 3
The Gibson approach opens the interval between the gluteus maximus and the tensor fascia lata. The greater trochanter is visualized and the sliding or Z-shaped osteotomy is prepared
Fig. 4
The capsule is incised in a Z-fashion in order to protect the retinacular vessels that penetrate the femoral head a distance of 4–5 mm from the postero-superior head neck junction
Fig. 5
The femoral head is dislocated and the view on the acetabulum is excellent from anterior to posterior. The transverse acetabular ligament is seen and is used as a landmark to fix the graft circumferentially. The labrum is hypoplastic and very thin. Therefore, the sealing function is expected to be insufficient
The hip joint is inspected and the labrum is then circumferentially detached from the acetabular rim. Most often the labrum is thinned and will not provide sufficient coverage of the head to ensure an adequate sealing function (Fig. 6). A semitendinosus allograft is used because it is long enough (8–15 cm), will be thick enough to provide adequate coverage, and is not associated with comorbidities of the graft harvesting. Therefore, the semitendinosus allograft is preferred to reconstruct the labrum. The graft is thawed and prepared during rim trimming. The length of the graft can be measured with the debrided labrum or with a pliable caliper. Both tendon ends are secured to an ACL-preparation kit with an absorbable suture (Vicryl 1) using a Krackow stitch. A tubular double loop is created using a baseball stitch with absorbable sutures (Vicryl 2/0). Both tendon strands are sewn to each other over the full length of the graft (Fig. 7).

 Neuromuscular Hip Disorders: Focus on Cerebral Palsy
Neuromuscular Hip Disorders: Focus on Cerebral Palsy
 Femoral Deformities: Varus, Valgus, Retroversion, and Anteversion
Femoral Deformities: Varus, Valgus, Retroversion, and Anteversion
 Surgical Technique: Arthroscopic Labral Management
Surgical Technique: Arthroscopic Labral Management
 Surgical Technique: Endoscopic Gluteus Medius Repair
Surgical Technique: Endoscopic Gluteus Medius Repair
 Introduction to Static and Dynamic Overload of Hip Pathology
Introduction to Static and Dynamic Overload of Hip Pathology
 Atraumatic Instability and Surgical Technique
Atraumatic Instability and Surgical Technique




Related posts:
Neuromuscular Hip Disorders: Focus on Cerebral Palsy
Femoral Deformities: Varus, Valgus, Retroversion, and Anteversion
Surgical Technique: Arthroscopic Labral Management
Surgical Technique: Endoscopic Gluteus Medius Repair
Introduction to Static and Dynamic Overload of Hip Pathology
Atraumatic Instability and Surgical Technique
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
