Study author(s)
Year
Journal title
Definition
Cerezal et al.
2012
Eur J Radiol
Inability to keep femoral head centered within acetabular fossa, without complete luxation or marked subluxation of the joint
Hip laxity is not equivalent to microinstability (presence of symptoms = microinstability)
Overuse and repetitive motion is most common cause of microinstability
Microinstability may lead to concomitant intra- and extra-articular injury
Domb et al.
2013
Arthroscopy
Microinstability may lead to ligamentum teres tears, large labral tears, and advanced acetabular chondral damage
Amenabar et al.
2012
Arthroscopy
Idiopathic instability that occurs in absence of trauma, dysplasia, overuse, or connective tissue disorder
Ligamentum teres has role as hip stabilizer and should be included in the evaluation of stability
Guanche et al.
2005
Arthroscopy
Eight elite runners (mean age 36 years) underwent hip arthroscopy for labral tear
Six subjects had Outerbridge Grade III acetabular articular cartilage injury
Three subjects had complete avulsions of the ligamentum teres
Theorize repetitive hyperextension during stride leads to “subtle instability” or “recurrent subluxation” and attritional stress at chondrolabral junction and ligamentum teres
Kolo et al.
2013
Skeletal Radiol
Professional ballet dancers
MRI-documented joint subluxation in all hips in the “splits” position with only 1/59 hips demonstrating cam or pincer FAI
In comparison to control, ballet dancers had significantly more acetabular chondral lesions, labral tears, and herniation pits
Relevant Anatomy
Capsulotomy is necessary to navigate the joint for both diagnostic and therapeutic purposes. However, many authors now contend that iatrogenic instability may result if the capsulotomy is not closed (Fig. 1). As the number of hip arthroscopies has increased dramatically (up to 18-fold) over the past decade [1], warranted concern has been emphasized in the size and type of capsulotomy performed and its routine closure [2]. Capsular preservation (minimal capsulotomy, routine closure) is encouraged for the retention of normal anatomy and optimizing outcomes. The iliofemoral ligament is the strongest of four discrete hip capsular ligaments (in addition to ischiofemoral, pubofemoral, zona orbicularis), and its primary purpose is to restrain anterior translation, with hip extension and external rotation. This static soft tissue stabilizer of the hip joint is disrupted during interportal (anterolateral to mid-anterior; Fig. 2) and “T” (Fig. 3) capsulotomies. Three recent cadaveric biomechanical studies (Table 2) have illustrated the importance of the iliofemoral ligament to the structural integrity of normal hip joint mechanics: Iliofemoral sectioning results in increased external rotation, extension, and anterior translation with no difference between the intact and repaired state [3–5].
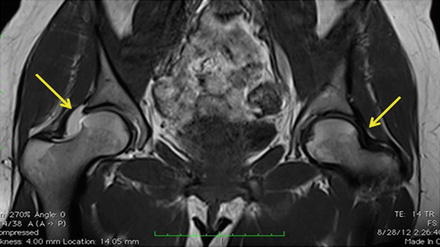
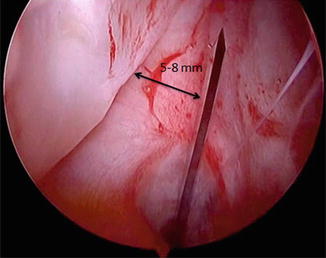
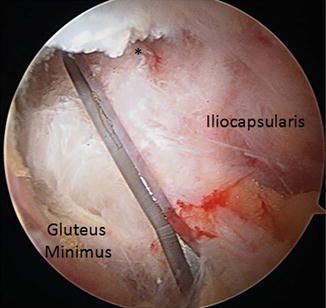
Fig. 1
T1-weighted coronal series right magnetic resonance hip arthrogram. In comparison to the normal left hip, the post-arthroscopic right hip (with capsulotomy left open) demonstrates capsular opening from the acetabular rim with dye extrusion (Modified from McCormick et al. [37] with kind permission from Springer Science and Business Media)
Fig. 2
Interportal capsulotomy. This incision is made in the right hip anterior capsule with the patient supine, in traction, using an arthroscopic scalpel, while viewing from anterolateral portal. It is important to leave a sufficient cuff of tissue on the acetabular side to repair at the conclusion of the case (Reprinted from Harris et al. [2] with permission from Elsevier)
Fig. 3
“T” capsulotomy. This incision is made in the right hip anterior capsule over the anterosuperior femoral neck with the patient supine, in traction, using an arthroscopic scalpel, while viewing from anterolateral portal. The iliocapsularis (medial) and gluteus minimus (lateral) are the anatomic landmarks used to make the “T” in the capsule, affording >180° visualization of the peripheral compartment for femoral head/neck cam osteochondroplasty (Reprinted from Harris et al. [2] with permission from Elsevier)
Table 2
Role of hip capsule in microinstability; IFL (iliofemoral ligament)
Study | Study design | Role |
|---|---|---|
Myers et al. [3] | Cadaveric biomechanical | Increased external rotation with IFL sectioning (increased 12.9°) (p <.0001) |
Fluoroscopy | Increased anterior translation with IFL sectioning (increased 1.8 mm) (p <.001) | |
No difference in external rotation or anterior translation between intact/repaired state | ||
Martin et al. [4] | Cadaveric biomechanical | Release of medial, lateral arms IFL gave greatest increase of external rotation |
Motion tracking | Lateral arm release provides more motion in flexion and neutral | |
Lateral arm release also provides more internal rotation, primarily in extension | ||
Hewitt et al. [5] | Cadaveric biomechanical | IFL much stronger than the ischiofemoral ligaments |
Load to failure | IFL greater stiffness than ischiofemoral ligaments | |
IFL greater tensile load to failure than ischiofemoral ligaments |
The ligamentum teres is a strong hip joint stabilizer (Table 3). It becomes taut with hip flexion, adduction, and external rotation. Despite its name “teres” (Latin for “round”), the ligament is actually triangular to flattened in shape for part of its intra-articular course (approximately 30–35 mm) [6]. Its diameter is highly variable and circumferentially covered with synovium. In the normal hip, the synovium is not highly vascular to the naked eye or with the arthroscope. However, in a hip with Legg-Calve-Perthes disease, the synovium and the ligament itself may be thicker with significant inflammation [7]. In a developmentally dysplastic hip, the ligament may be abnormally hypertrophic (thicker, longer) [7]. In traumatic ligamentum teres ruptures, the acetabular side tears before the femoral side and intra-substance tears are rare [8].
Table 3
Role of ligamentum teres in instability; CEA (center-edge angle)
Study author(s) | Year | Journal title | Role |
|---|---|---|---|
Domb et al. | 2013 | Arthroscopy | Ligamentum teres tear risk factors assessed in 463 hips undergoing arthroscopy |
Hips with low lateral coverage index (lateral CEA – acetabular inclination) 1.74 times more likely to have ligamentum tear than those with high lateral coverage index | |||
Significantly greater number of ligamentum tears when labral tear extended posterior to 11 o’clock or anterior to 4 o’clock | |||
Significantly more advanced acetabular chondral damage seen in ligamentum tears | |||
Ligamentum teres tears speculated to be a sign of microinstability | |||
Cerezal et al. | 2012 | Eur J Radiol | Stabilizer in adduction, flexion, external rotation |
Ligamentum teres tear may lead to microinstability | |||
Microinstability may lead to ligamentum teres tear | |||
Haviv et al. | 2011 | Knee Surg Sports Traumatol Arthrosc | Arthroscopic debridement of 29 hips with isolated partial ligamentum teres tear provides significant pain relief and improvement in function |
High risk of recurrence associated with ligamentous laxity | |||
Partial ruptures are due to repetitive stretching and may be seen in isolation – mostly in young female gymnasts, dancers, and with calisthenics | |||
Amenabar et al. | 2012 | Arthroscopy | Case report of young female with persistent pain after ligamentum debridement, anterior capsulorrhaphy. Underwent ligamentum reconstruction using semitendinosus autograft |
Successful 12-month outcome, but new lateral pain over suture knot at 15 months | |||
Repeat arthroscopy showed reconstruction sutures intact, but graft resorption |
The ligamentum teres originates from the transverse acetabular ligament and spans the bony junction of the ischium-pubis from the 5 to 7 o’clock position on the acetabular clock face. It inserts on the femoral side at the anterosuperior aspect of the fovea capitis, which is a bare area without articular cartilage, located posteroinferiorly on the femoral head. Within the ligament is the artery of the ligamentum teres, a branch usually derived from the posterior division of the obturator artery and less commonly from the acetabular branch of the medial femoral circumflex artery (medial epiphyseal artery). Regardless of its source, the amount of vascularity supplied to the femoral epiphysis is variable and minimal.
Relevant Pathophysiology
The presence of microinstability does not preclude other concomitant intra- and extra-articular disorders. In fact, subtle instability may actually increase the stress response and potential damage to local structures including labrum, articular cartilage and underlying subchondral bone, ligamentum teres, iliopsoas tendon, iliotibial band, hip abductors, and the remaining normal capsule [9]. Further, FAI symptoms may be exacerbated due to the excessive motion [10]. Conversely, impingement may actually induce instability in the following four ways: (1) Excessive acetabular anteversion can result in anterior hip instability and posterior acetabular rim impingement; (2) excessive acetabular retroversion can result in anterior impingement and posterior instability; (3) excessive femoral anteversion can result in anterior hip instability and posterior acetabular rim impingement; (4) excessive femoral retroversion can result in anterior impingement and posterior instability. In a study that examined the association between arthroscopic iliopsoas tenotomy and femoral version, significantly worse outcomes were observed in subjects with greater degrees of femoral anteversion (>25°) due to the loss of the anterior dynamic stabilizing effect performed by the iliopsoas [11].
Cam impingement prohibits true ball-and-socket mechanics, thus causing anterior levering over the rim (fulcrum) with subsequent posterior instability [12]. With traumatic posterior hip dislocation, there is a greater prevalence of anterior cams and femoral retroversion than in normal hips [13]. In an exclusively athletic population with low-energy subluxation or dislocation and posterior acetabular rim fracture, cam and/or pincer impingement has been identified in 64–82 % of subjects [14–16]. In athletes with larger degrees of motion (such as ballet, dancing, gymnasts), there may be impingement-induced instability without abnormal cam or pincer deformities. In a cohort of 59 professional ballet dancers, only one hip had evidence of a cam deformity, while several other abnormalities were identified on magnetic resonance imaging due to a dynamic “pincer” mechanism from the extreme motion involved with their sport [17]. Further, while in the “splits” position, all hips subluxated (mean 2.1 mm). In comparison to a control group, the abnormalities in ballet included significantly more acetabular cartilage lesions (mostly superior), more labral tears (mostly posterosuperior to anterosuperior), and more superior herniation pits. Despite the latter study’s prevalence of imaging abnormalities, less than two-thirds of subjects were symptomatic at the time imaging was performed in a follow-up investigation [18]. Further, when examining certain ballet positions, the mean translation was up to 4.6 mm (6.4 mm in one subject) [19]. Whether or not the microinstability observed in these studies (with the associated intra-articular pathologies) will lead to early osteoarthritis is yet to be determined.
Discrete frank hip dislocation is at the end of the microinstability spectrum. In the postoperative setting, instability may occur along this spectrum to variable degrees. Nine cases of post-arthroscopic iatrogenic hip dislocation have been presented in the literature [10, 20–25]. Due to publication bias, this is likely a significant underestimate of the true incidence of instability following hip arthroscopy. Thus, many authors have subsequently recommended routine capsular closure during arthroscopy, which has both potential advantages and disadvantages (Table 4) [2]. The following patient-, hip-, and surgical technique-specific factors have been associated with this uncommon, but serious, complication: capsulotomy or capsulectomy without repair, labral resection (versus repair or refixation), aggressive acetabuloplasty rim trimming in dysplastic configurations, and overall capsular laxity [26]. In this situation, revision surgery (either arthroscopic or open) for capsulorrhaphy may be indicated.
Table 4
Advantages and disadvantages of capsular closure during hip arthroscopy
Complete capsular repair or plication | Leaving capsulotomy open |
|---|---|
Advantages | Advantages |
Retention of hip stability | May be therapeutic (pre-op tight anterior capsule) |
External rotation, anterior translation | Reduced surgical time |
Prevention of iatrogenic subluxation, dislocation | No risk of overtightening anterior capsule and subsequent loss of motion |
Prevention of edge loading of repaired labrum | |
No loss of motion | |
Disadvantages | Disadvantages |
Technically demanding, may damage articular surfaces | May lead to iatrogenic instability, especially in ligamentously lax hypermobile individuals and in sport-specific athletes |
Multiple nonabsorbable sutures in anterior capsule | Exacerbated during excessive femoral osseous resection |
Increased surgical time |
In addition to the capsule, other structures may be pathologically involved in microinstability. Ligamentum teres ruptures may be a sign of microinstability, or they may cause microinstability. Two classification systems exist to categorize these injuries (Table 5) [27, 28]. The more recently defined classification, a descriptive classification, was published in a level IV evidence retrospective case series of 616 arthroscopies in which 51 % had ligamentum teres ruptures [28]. It was observed that patients with tears had significantly greater range of motion, less lateral acetabular coverage, larger labral tears, and more advanced acetabular articular cartilage damage [28, 29]. Despite the possible role that the ligamentum teres may play in hip stability, counter to this argument is that it is commonplace for the ligament to be resected during open surgical dislocation femoral osteochondroplasty without residual instability following surgery. However, close history and examination does reveal that these patients do have subtle instability, similar to that of a partial (Gray and Villar Type II) ligamentum rupture, rather than a complete (Type I) rupture [30]. In addition to the capsuloligamentous structures, the musculotendinous dynamic structures that cross the joint may be weak, potentially altering the axial/appendicular skeleton mechanics and leaving the joint less stable.
Table 5
 Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum




Ligamentum teres tear classification systems
Related posts:
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
