Fig. 1
Intraoperative image of a right hip demonstrating the placement of the anterolateral (AL), mid-anterior (MA), distal anterolateral accessory (DALA), posterolateral (PL), and proximal anterolateral accessory (PALA) portals for use in the peritrochanteric space. Anterior superior iliac spine (Black arrow; ASIS). Greater Trochanter (G.T.)
After the peritrochanteric space has been accessed, visualization is achieved with a 70° arthroscope in the mid-anterior portal. Diagnostic evaluation begins with visualization of the gluteus maximus tendon distally as it inserts on the femur just below the vastus lateralis (Fig. 2). Exploration posterior to the tendon is cautioned to avoid injury to the sciatic nerve. The camera is then directed towards the lateral femur and the longitudinal fibers of the vastus lateralis. The tendinous insertion and muscle of the gluteus medius is identified as the camera is moved further proximal. Inspection of the peritrochanteric space is complete as the iliotibial band is identified by looking proximal and lateral.

Fig. 2
Intraoperative image of a left hip demonstrating the probe at the insertion of the gluteus maximus tendon to the posterior portion of the femur. This is the distal extent of the peritrochanteric space
Additional authors have reported alternative portals to access the peritrochanteric space in order to perform a trochanteric bursectomy and or iliotibial band lengthening [16–20]. Farr et al. described a technique involving two incisions: one 4 cm proximal to the greater trochanter along the anterior border of the iliotibial band and the other 4 cm distal and along the posterior border. A 30° arthroscope was introduced through the distal portal for viewing while the proximal portal was used as the working portal [20].
A thorough trochanteric bursectomy is performed first (Fig. 3). A spinal needle is placed under direct visualization 4–5 cm distal to the anterolateral portal to create a distal anterolateral accessory portal. The arthroscopic shaver is inserted through this portal, and a thorough trochanteric bursectomy is performed over the distal portion of the space. The bursectomy is performed from distal to proximal. Thickened bursal tissue and fibrinous bands are cleared off of the gluteus maximus tendinous insertion distally. A second accessory portal is created 2–3 cm proximal to the anterolateral portal called the proximal anterolateral accessory portal to remove the most proximal portions of the inflamed bursal tissue. Arthroscopic electrocautery can also be used to cauterize bursal vessels and complete the bursectomy.
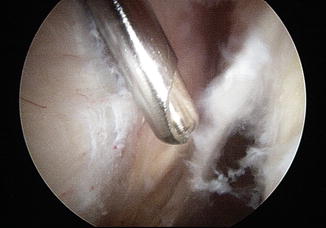
Fig. 3
Intraoperative image of a left hip demonstrating thick bands of trochanteric bursa tissue removed by the arthroscopic shaver. The vastus lateralis is to the left
If concomitant symptomatic external “snapping hip” or coxa saltans is present, lengthening of the iliotibial band is performed. A beaver blade or arthroscopic cautery device is used to create a transverse or cruciate-style lengthening of the iliotibial band [9, 12, 18].
Gluteus Medius Repair
Prior to repair of the hip abductor tendons, it is important to understand the anatomy and insertional footprint of the gluteus medius and minimus. Robertson et al. described the anatomy and dimensions of the abductor footprint insertion in a cadaveric study [21]. The four facets of the greater trochanter include the anterior, lateral, superoposterior, and posterior facets. The gluteus medius inserts onto the superoposterior and lateral facets of the trochanter, with the most robust portion of the tendon inserting on the superoposterior facet in a circular footprint pattern. The superoposterior insertion has a circular shape with an approximate diameter of 17 mm and a mean area of insertion of 196.5 mm2, while the lateral facet footprint is approximately 35 mm long and 11 mm wide with a mean area of insertion of 438.0 mm2. The gluteus minimus originates on the outside of the ilium between the anterior and inferior gluteal lines and from the sciatic notch, where the muscle protects the superior gluteal nerve and artery. The gluteus minimus has a broad insertion running from the hip capsule anterosuperiorly to its major insertion on the anterior facet of the greater trochanter deep to the gluteus medius. A bald spot of the trochanter, where there are no distinct tendon insertions, exists between the insertion of the gluteus minimus on the anterior facet and the gluteus medius on the lateral facet. The posterior facet of the greater trochanter lacks a tendon insertion and lies posterior to the lateral facet and inferior to the superoposterior facet with the trochanteric bursa overlying it.
Slight traction of the hip is needed to place the gluteus medius muscle fibers on tension in order to delineate proximal bursal tissue from gluteus medius muscle fibers. The 70° arthroscope is placed in the proximal anterolateral accessory portal to achieve a more global view of the abductors, while the working instruments can be placed in the mid-anterior and distal anterolateral accessory portal. The tears can be classified as intrasubstance, partial thickness, or full thickness [7, 8, 15, 21]. The tear location is often on the undersurface analogous to an articular sided rotator cuff tear, which extends posteriorly demonstrating a full-thickness tear.
Endoscopic techniques and fundamentals for gluteus tendon repair are analogous to rotator cuff repairs with the goal of a secure, tension-free repair, with restoration of the tendon footprint.
After the tendon is identified, the torn edge of the tendon is gently debrided to stable tissue. Next, a grasper is used to manually reduce the tear to its anatomic position on the footprint. An arthroscopic burr is used to decorticate the greater tuberosity footprint to a bleeding base (Fig. 4). A spinal needle is placed to localize the best angle for anchor placement. Bioabsorbable or metallic suture anchors are then inserted into the footprint. Fluoroscopic guidance is useful to confirm proper anatomic positioning of the anchors.
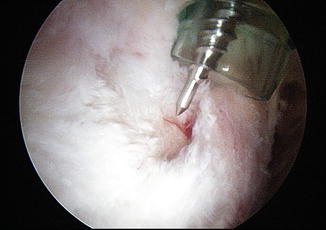
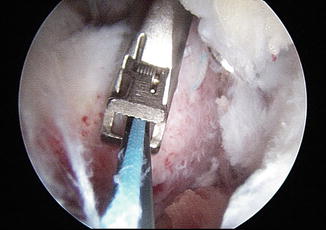
Fig. 4
Intraoperative image of a left hip demonstrating a longitudinal tear in the gluteus medius tendon. The footprint has been decorticated in preparation for anchor placement. An awl is utilized to prepare a pilot whole for the anchor
Arthroscopic plastic cannulas 7–8.25 mm in size are then inserted through the working portals for instrumentation and suture management. A suture-passing device is used to pass suture through the tendon from posterior to anterior sequentially. Voos et al. described using single- or double-loaded suture anchors with passage of sutures in a simple fashion [7, 9]. Domb et al. published a technique for repair of partial-thickness undersurface gluteus medius tendon tears [8, 14]. In the technique described by Domb et al., a beaver blade is used to fashion a longitudinal split in the midsubstance of the lateral facet insertion of the gluteus medius. Through this split, the undersurface tearing and pathologic tendon tissue can be assessed. A suture passer used to pass one limb of each suture through the anterior part of the tendon and one limb of each suture through the posterior part. The steps may be repeated with a second anchor if necessary. This technique results in a side-to-side repair of the longitudinal tendon split. An arthroscopic suture-passing device that retrieves the suture (Fig. 5) such as the Scorpion (Arthrex Naples, Florida) and suture penetrators (Fig. 6) assists in ease of maneuvering in the peritrochanteric space.
 Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum




Related posts:
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
