Fig. 1
Exposure of the femoral head (F), labrum (L), and acetabular rim (A), with probing of the labrum using a nerve hook to determine labral pathology
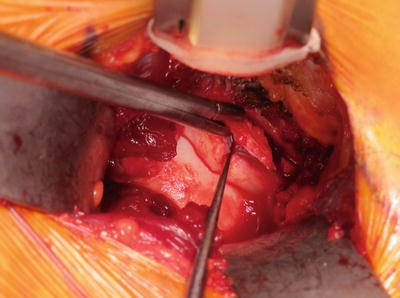
Fig. 2
Calcified labral lesions are carefully excised after the labrum is exposed
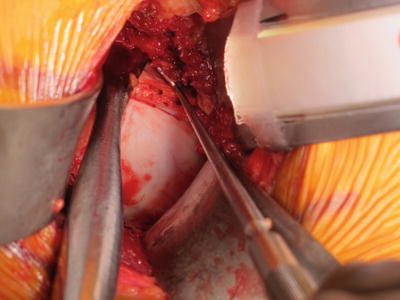
Fig. 3
Longitudinal traction on the limb allows a blunt Cobb elevator to be inserted into the joint. This aids exposure of the cartilaginous surfaces allowing a nerve hook to be used to gently probe any chondral flaps
Acetabular Rim Debridement
Inspection and assessment of the articular cartilage of the femoral head and acetabulum is now performed using a nerve hook to gently probe the surfaces for chondral flaps (Fig. 3). Occasionally, in the presence of a significant full-thickness flap, micro-fracturing is performed. The acetabular rim can now be addressed. If over-coverage of the femoral head by the acetabular rim is present, as a result of acetabular retroversion, this redundant or excess rim can be excised. A 10 mm curved osteotome in combination with a 5 mm pneumatic burr is used to achieve adequate debridement. The amount of debridement varies depending on the extent of the chondral lesion, but care must be taken not to remove more than 1 cm from the rim as this may lead to joint instability postoperatively.
Femoral Neck Osteoplasty
Next the femoral head-neck junction is examined. When a cam-type lesion is present, it is usually located on the anterosuperior region of the neck and often exhibits a characteristic reddish appearance. The assistant should now place the hip in internal rotation, which simulates the impingement test and allows the surgeon to clearly define the extent of the cam lesion (Fig. 4). It is now imperative to define the head-neck junction and also to denude the cam-type lesion of its cartilage covering. Now the neck osteoplasty can be safely performed, again using the 10 mm osteotome and the 5 mm burr. The osteoplasty is only complete when once again the smooth contour of the femoral head and neck is recreated. The preoperative decision regarding the extent of the resection can be difficult as FAI is a dynamic process. The resection should always be less than 30 % of the neck area [4]. A reference guide to the desired resection based on the anteroposterior radiograph of the pelvis starts the bony correction 15 mm away from the acetabular rim, with extension of it 10 mm anterior to the 12 o’clock position and 10 mm to the lateral border (Fig. 5). On the Lowenstein lateral view, a resection depth of 5 mm is acceptable to restore the femoral head-neck offset, with extension distally in the axial plane of up to 20 mm. The adequacy of the neck osteoplasty is assessed by once again performing internal rotation of the limb to simulate the impingement test, with absence of impingement signifying sufficient resection (Fig. 4). The surgeon should aim to get hip flexion of 100° and internal rotation of 15° without impingement occurring. Three-dimensional assessment of the neck osteoplasty can be performed at the time of surgery. Computer-assisted osteoplasty has been described to aid with the desired level of resection [5–7]; however this should not be solely relied upon.

 Neuromuscular Hip Disorders: Focus on Cerebral Palsy
Neuromuscular Hip Disorders: Focus on Cerebral Palsy
 Femoral Deformities: Varus, Valgus, Retroversion, and Anteversion
Femoral Deformities: Varus, Valgus, Retroversion, and Anteversion
 Rehabilitation of Non-Operative Hip Conditions
Rehabilitation of Non-Operative Hip Conditions
 Surgical Technique: Open Proximal Hamstring Repair
Surgical Technique: Open Proximal Hamstring Repair
 Subspine Impingement and Surgical Technique
Subspine Impingement and Surgical Technique
 Atraumatic Instability and Surgical Technique
Atraumatic Instability and Surgical Technique




Related posts:
Neuromuscular Hip Disorders: Focus on Cerebral Palsy
Femoral Deformities: Varus, Valgus, Retroversion, and Anteversion
Rehabilitation of Non-Operative Hip Conditions
Surgical Technique: Open Proximal Hamstring Repair
Subspine Impingement and Surgical Technique
Atraumatic Instability and Surgical Technique
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
