Fig. 1
The wave or carpet sign (Source: Mr. Giles Stafford)

Fig. 2
Stable labrum (Source: Mr. Giles Stafford)
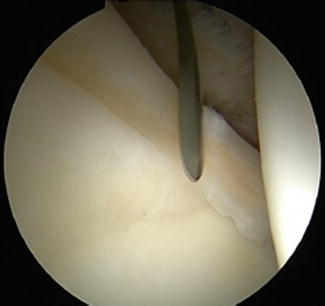
Fig. 3
Arthroscopic knife gaining access to delaminated cartilage (Source: Mr. Giles Stafford)
The microfracture awl is passed under the labrum into the pocket and the microfracture technique is performed on the underlying subchondral bone (Fig. 4). Care must be taken to ensure that no further damage occurs to the cartilage.

Fig. 4
Microfracture to subchondral bone (Source: Mr. Giles Stafford)
The application of the fibrin glue requires two arthroscopy needles. The first is into the pocket behind the delaminated cartilage for application of the fibrin (Fig. 5). Another needle is inserted through the anterolateral portal into the base of the central compartment or cotyloid fossa for aspiration of the joint to dryness (Fig. 6). Once the irrigation fluid is removed (Fig. 7), the fibrin glue may be applied using the first needle (Fig. 8). Immediately following this, an angled arthroscopic punch is used to press firmly on the delaminated cartilage to ensure it securely adheres to subchondral bone while the fibrin glue sets (Fig. 9). The process of bonding the cartilage to the bone takes 2 min, resulting in a successful repair (Fig. 10). Any excess adhesive that spills into the central compartment can be removed using arthroscopic graspers.
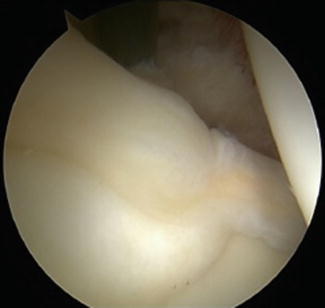
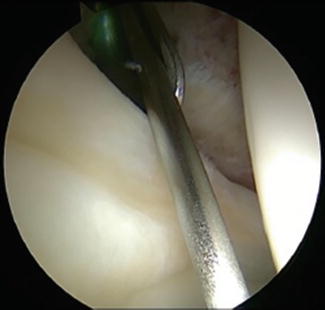



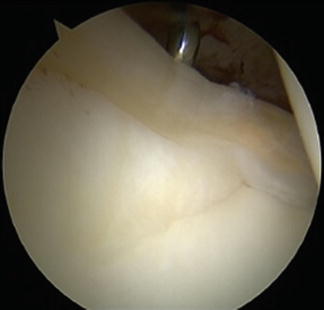
Fig. 5
Needle to access “the pocket” (Source: Mr. Giles Stafford)
Fig. 6
Use of needle to aspirate joint fluid, located in the cotyloid fossa (Source: Mr. Giles Stafford)
Fig. 7
Needle insertion into the pocket behind the labrum (Source: Mr. Giles Stafford)
Fig. 8
Application of fibrin glue using the needle in “the pocket” (Source: Mr. Giles Stafford)
Fig. 9
Arthroscopic punch used to apply pressure to the cartilage to ensure adhesion between the cartilage and subchondral bone (Source: Mr. Giles Stafford)
Fig. 10
Successful repair following fibrin glue adhesion (Source: Mr. Giles Stafford)
Reduction of the femoral head into the acetabulum results in further compression of the cartilage onto the subchondral bone. Postoperatively the patients are discharged after physiotherapy review and implementation of a rehabilitation regime with adequate analgesia.
Results in the Literature
Results are limited to a case series of 43 patients followed up at 1 and 3 years. Patients were clinically assessed pre- and postoperatively using the Modified Harris Hip Score, and these results are statistically analyzed.
At 28 months there was a statistically significant improvement in pain from a mean of 21.8 (95 % CI 19–24.7) pre-operatively to 35.8 (95 % CI 32.6–38.9). A more modest statistically significant improvement in function was also demonstrated [3].
Three patients underwent revision hip arthroscopy surgery for iliopsoas pathology. The repaired articular cartilage in these patients was inspected and appeared to be in good condition, suggesting that this method is effective in the treatment of delaminated cartilage [3].
The Future
A small case number and no reported histological analysis of the repaired cartilage limit the above study. Therefore, to further validate this as an effective method of repair, a double-blinded randomized controlled trial would be required. Biopsy of the macroscopically healthy cartilage may be viewed as ethically complicated. Therefore, a less invasive method of assessing the health of the cartilage using image novel MRI techniques include dGEMRIC (delayed gadolinium-enhanced MRI of cartilage) and T2 cartilage mapping, both of which are currently being validated with regard to the measurement of cartilage quality [40, 41, 42].
There are developments in fibrin glue, which may improve the efficacy of the healing process. In addition adhesive and hemostatic properties studies have shown fibrin glue is also a useful vehicle for the delivery of mesenchymal stem cells which results in earlier healing of meniscal injuries in animal models and improved healing in other areas of medicine [43–47].
Overall, fibrin glue as an adjunct to microfracture has been shown to be safe and effective in the management of cartilage delamination with equivalent and possibly superior results to traditional methods involving excision of cartilage with microfracture alone.
Summary
In summary this chapter outlines the history of fibrin and its properties, both hemostatic and adhesive. Furthermore, the technique whereby delaminated cartilage is adhered back to its subchondral bone using fibrin glue is described. The fibrin also has effects at a cellular level to stimulate the repopulation of the cartilage with chondrocytes and therefore results in healthy cartilage. This technique has been shown to be effective in improving Harris Hip Scores and halt progression of hyaline cartilage damage.
References
1.
Tzaveas AP, Villar RN. Arthroscopic repair of acetabular chondral delamination with fibrin adhesive. Hip Int. 2010;20(1):115–9.PubMed
2.
Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. Anterior femoroacetabular impingement: part II. Midterm results of surgical treatment. Clin Orthop Relat Res. 2004;418:67–73.
3.
4.
Hubbard MJ. Arthroscopic surgery for chondral flaps in the knee. J Bone Joint Surg. 1987;69:794–6.
5.
Miller BS, Steadman JR, Briggs KK, Rodrigo JJ, Rodkey WG. Patient satisfaction and outcome after microfracture of the degenerative knee. J Knee Surg. 2004;17(1):13–7.PubMed
6.
Related posts:
 Neuromuscular Hip Disorders: Focus on Cerebral Palsy
Neuromuscular Hip Disorders: Focus on Cerebral Palsy
 Femoral Deformities: Varus, Valgus, Retroversion, and Anteversion
Femoral Deformities: Varus, Valgus, Retroversion, and Anteversion
 Surgical Technique: Arthroscopic Labral Management
Surgical Technique: Arthroscopic Labral Management
 Surgical Technique: Endoscopic Gluteus Medius Repair
Surgical Technique: Endoscopic Gluteus Medius Repair
 Introduction to Static and Dynamic Overload of Hip Pathology
Introduction to Static and Dynamic Overload of Hip Pathology
 Atraumatic Instability and Surgical Technique
Atraumatic Instability and Surgical Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


