Fig. 1
Portal placement for trochanteric bursectomy. A preferred technique is to use the anterolateral portal and the DALA portal. Other portals can be used according to surgeon preference
Diagnostic Arthroscopy and Bursectomy
Once the initial AL portal is established, a diagnostic arthroscopy is performed with a 70° arthroscope. Initially the camera and light source is directed inferiorly, and the insertion of the gluteus maximus tendon under the vastus lateralis is identified; this will be the distal extent of the bursectomy (Fig. 2). An initial bursectomy may be required to maximize visualization of this structure. There are three bursas that have been described, and a thorough bursectomy requires that the subgluteus maximus bursa, the subgluteus medius bursa, and the gluteus minimus bursa are all debrided (Fig. 3). The camera is then directed toward the femur and moved proximally; this will bring the longitudinal fibers of the vastus lateralis into view. The fibers of the vastus lateralis can then be traced up to the insertion at the vastus tubercle. By looking immediately anterior to this structure, the anterior facet of the greater trochanter can be easily identified, as can be the insertions of the gluteus medius and minimus [10, 11, 13].
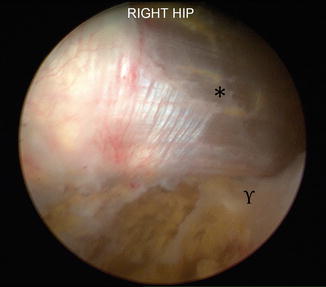
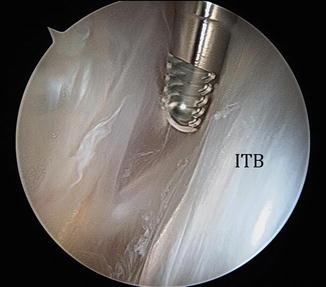
Fig. 2
Distal extent of the peritrochanteric space. * vastus lateralis, ϒ gluteus maximus insertion
Fig. 3
Bursa in the peritrochanteric space. ITB iliotibial band
A thorough bursectomy is complete when it extends to the insertion of the gluteus maximus and when the gluteus medius and minimus insertions are clearly visualized (Fig. 4). This step is accomplished with a motorized shaver and a radiofrequency device to maintain hemostasis. In addition to a thorough bursectomy, the posterior third of the ITB will often be released (Video 1). There is evidence that this portion of the procedure can be beneficial in cases where direct wear on the greater trochanter is seen or in patients with known recalcitrant external snapping hip symptoms [11]. This can be performed with either a radiofrequency device, a beaver blade, or a shaver.
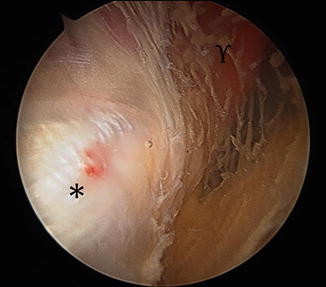
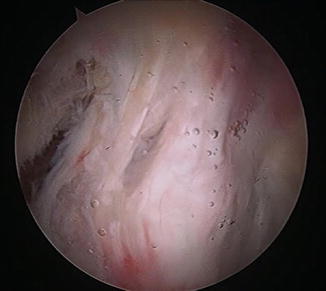
Fig. 4
Proximal extent of the peritrochanteric space. * gluteus medius tendons, ϒ gluteus medius muscle belly
Video 1
Appearance of the peritrochanteric space after a complete bursectomy
Results
Few studies are available that assess the effectiveness of this procedure. Release of the posterior third of the ITB in conjunction with bursectomy has been shown to have favorable results [11, 16]. In a prospective study of 25 patients, Baker et al. showed significant improvement in visual analog pain scores, Harris hip scores, and improvements in SF 36 [10]. As previously described, calcifications can be seen within the gluteal tendons in a similar manner as calcific tendonitis of the rotator cuff. Kandemir has demonstrated effective treatment of this condition with debridement of the calcific deposits and bursectomy for the diagnosis of GTB [17].
Summary
GTB is a very common condition that can be difficult to treat. As it is a diagnosis of exclusion, a thorough and detailed work-up of all associated conditions must be performed. Nonoperative therapy is often quite effective in managing this condition, but when conservative measures fail to produce long-term benefit, surgical intervention can be a reliable and successful treatment in the properly indicated patient.
Related posts:
 Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Complications with Hip Arthroscopy and Open Hip Surgery
Surgical Technique: Arthroscopic Treatment of Chronic Slipped Capital Femoral Epiphysis
Smith-Petersen Approach to the Hip
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Complications with Hip Arthroscopy and Open Hip Surgery
Surgical Technique: Arthroscopic Treatment of Chronic Slipped Capital Femoral Epiphysis
Smith-Petersen Approach to the Hip
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


