Fig. 1
The patient is positioned in the lateral decubitus position with the entire hip and leg draped free. Proximal and distal portals are marked on the skin, and a spinal needle marks the trochanteric prominence
Next, two portals are created: a proximal portal is made approximately 2–3 cm proximal to the most superior aspect of the greater trochanter and a distal portal is made 2–3 cm distal to the trochanteric prominence. The portals are made in line with the needle, slightly anterior to the midpoint, and parallel to the fibers of the IT tract. A 4-mm, 30° arthroscope is then inserted into the subcutaneous tissues directly above the iliotibial band (ITB). A 4.5-mm shaver is inserted into the other portal aiming toward the superior tip of the greater trochanter using triangulation to find the spinal needle. The subcutaneous fat immediately adjacent and adherent to the ITB over the greater trochanter is cleared by the use of the 4.5-mm shaver. Alternatively, an arthroscopic ablator can be used to clear the subcutaneous fat or a combination of shaver and ablator can be used depending on the preference of the surgeon (Figs. 2 and 3). When the ITB can be well visualized, an approximately 5–6-cm longitudinal incision is made with the ablator in line with the ITB fibers slightly posterior to the midportion of the band and the trochanteric prominence (Figs. 4 and 5). This incision exposes the trochanteric bursa. The surgical assistant abducts the leg to further relax the incised ITB and to allow the arthroscope and instruments to be advanced underneath the ITB. A common pitfall is to make the incision too posterior, making it difficult to access the bursa properly. Using the spinal needle to localize the most prominent aspect of the trochanter and completely expose the ITB prior to making the split helps to prevent this problem. If muscle is visualized while making the ITB incision, the surgeon is too posterior and should reassess for proper position.
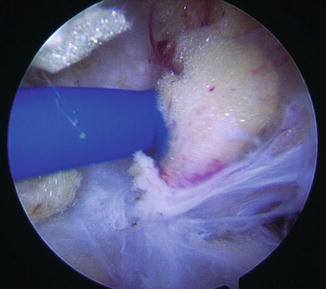
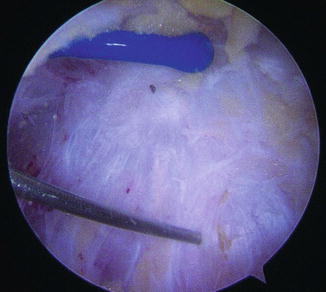
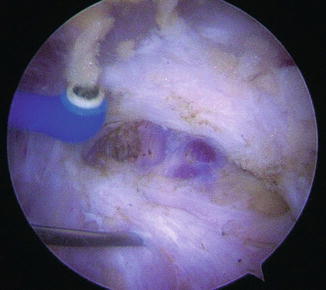
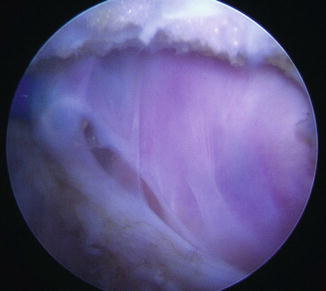
Fig. 2
An arthroscopic ablator is utilized to clear the subcutaneous fat from the underlying iliotibial band
Fig. 3
The iliotibial band is exposed. The spinal needle localizes the most prominent aspect of the greater trochanter
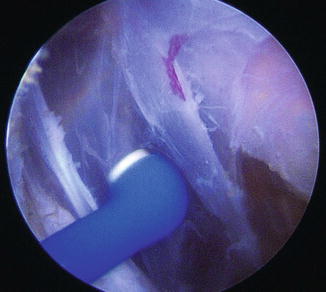
Fig. 4
The arthroscopic ablator is utilized to incise the iliotibial band in line with its fibers
Fig. 5
The iliotibial band is incised for a length of 5–6 cm to expose the trochanteric bursa
The bursa and its thick fibrous bands and adhesions are now able to be easily visualized. Debridement of these bands and bursal tissue is performed with the arthroscopic shaver and primarily with the arthroscopic ablator (Fig. 6). Coagulation with the ablator is frequently necessary to maintain hemostasis and visualization. The assistant slowly internally and externally rotates the abducted leg to expose the posterior and anterior portions of the bursa, respectively. Care must be taken with extreme internal rotation because this places the sciatic nerve at risk.
 Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum




Related posts:
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
