Fig. 1
Normal anatomy of hamstring origin on ischium (a) Cadaveric dissection of the ischium in a right hip, viewed from the posterior aspect (Note the everted tendon of the biceps/semitendinosus (B/ST) that is elevated and retracted laterally. SN Sciatic nerve). (b) Axial T2 weighted magnetic resonance image depicting the anatomy of the hamstring origin in a left hip. SM Origin of semimembranosus, B Biceps origin, ST Semitendinosus
Most acute injuries usually involve a traumatic event that includes forced hip flexion and knee extension. Most commonly, this has been described in waterskiing [9, 10]. However, the injury can result from any sporting activity that involves rapid acceleration and deceleration [10, 11].
Proximal hamstring tears can be categorized as complete avulsions, partial avulsions, apophyseal avulsions, and degenerative (tendinosis) avulsions [11]. Degenerative tears of the hamstring origin are insidious in onset and are commonly seen as an overuse injury, especially in runners. The mechanism of injury, presumably, is repetitive irritation of the medial aspect of the hamstring tendon (along the lateral aspect of the tuberosity, where the bursa resides). This causes an attritional tear of the tendon and chronic pain.
Commonly, athletes with proximal hamstring tendon tears describe a popping or tearing sensation with associated acute pain and bruising over the posterior hip and thigh [12, 13]. Occasionally, patients who present with either acute or chronic tears may complain of a pin and needle sensation in the sciatic nerve distribution [13, 14]. This may be due to acute compression from hematoma in the proximity of the sciatic nerve, acute traction-type injury in addition to the tendinous rupture, or chronic scarring and tethering of the tendon to the nerve. Similarly, symptoms of ischial bursitis include buttock or hip pain, as well as localized tenderness overlying the ischial tuberosity. Additional symptoms of chronic ischial bursitis may include tingling into the buttock with radiation down the leg [13].
Advanced imaging is crucial to obtain in cases of partial tears with chronic pain. Standard radiographs of the pelvis and a lateral of the affected hip are performed first to rule out any bony problems, in particular apophyseal avulsions of the ischial tuberosity in younger patients (Fig. 2). Most commonly, no fractures are identified and MRI is utilized to assess the proximal hamstring origin. A complete rupture of all three tendons is common and easily identified on MRI.

Fig. 2
AP radiograph of right hip showing a bony avulsion of the ischial tuberosity (arrow) in a 13-year-old runner
Partial hamstring origin tears , however, are more difficult to discern. For two tendon tears, which commonly have an associated musculotendinous junction injury to the third tendon (semimembranosus), this is especially difficult. Most commonly, there is an avulsion of the common semitendinosus and biceps origin, with the semimembranosus remaining intact [7]. In addition, partial tears without any significant retraction can be seen on MRI as a sickle sign and are partial avulsions of the semimembranosus (Fig. 3).
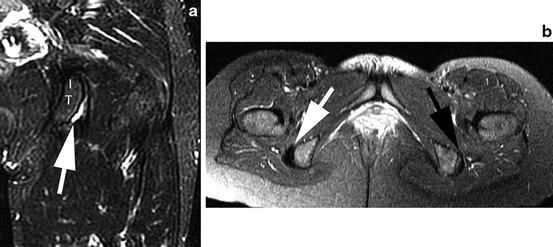
Fig. 3
MRI views of a partial insertional tear with a sickle sign, indicating fluid within the ischial bursa. (a) A coronal T2 weighted view of a right hip showing the sickle sign (white arrow). IT Ischial tuberosity. (b) Axial T2 weighted view showing both ischial tuberosities (Note the side with the black arrow showing the sickle sign and the normal side for comparison (white arrow))
Nonoperative treatment is most commonly recommended in the setting of low-grade partial tears and insertional tendinosis. Initial treatment consists of relative rest, oral nonsteroidal anti-inflammatory medications, and a physical therapy regime [15]. An ultrasound-guided corticosteroid injection may be used and has been shown to provide initial relief in up to 50 % of patients at 1 month [16]. Although evidence is lacking, platelet rich plasma (PRP) injections might also be considered for recalcitrant cases. Partial tears that remain symptomatic may benefit from surgical debridement and repair, similar to other commonly seen partial tendon tears (patella, quadriceps, and biceps) [17].
There are several series and descriptions of open surgical techniques [12, 13, 18–22]. To date, there has been no report of endoscopic management of these injuries. After developing experience in the open management of these injuries, the author has developed an endoscopic technique that allows a safe approach to the pathologic area. The benefits of this endoscopic approach include avoiding the need for excessive retraction or splitting the gluteus maximus and the use of endoscopic magnification to identify and protect the sciatic nerve. This technique with its inherent advantages may improve the management of these injuries and reduce morbidity.
Surgical Technique
The patient is positioned prone on a standard table that is flat. Bolsters are placed under the chest to support the torso. No effort is made to flex the hips, as this may decrease the potential distance between the ischium and the gluteus maximus, thus obliterating the potential working space. The posterior aspect of the hip is then draped assuring that the leg and thigh are free and can be freely manipulated during the procedure (Fig. 4).
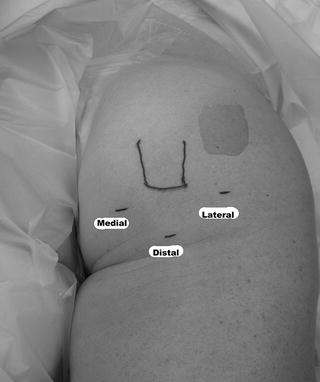
Fig. 4
The patient is positioned prone with the left hip and leg draped free. The outlined prominence is the palpable ischial tuberosity
Two portals are created; they are 2 cm medial and lateral to the palpable ischial tuberosity (Fig. 5). A blunt arthroscopic cannula is inserted into the lateral portal and a blunt switching stick in the medial portal. The instruments aim to localize the most prominent aspect of the ischium where the sciatic nerve is furthest away. The lateral portal is first used for the arthroscope and the plane between the gluteus maximus and ischium is developed. The prominence of the ischial tuberosity is identified and the medial and lateral borders are delineated. A 30° arthroscope is employed from the lateral portal and an electrocautery device is placed in the medial portal. Any remaining fibrous attachments between the ischium and the gluteus muscle are released, staying along the central and medial portions of the ischium to avoid coming near the sciatic nerve, which is well lateral (and anterior) to the ischial prominence. Once the tip and medial aspect of the ischium are delineated, the lateral aspect is then exposed with the use of a switching stick as a soft tissue dissector. With the lateral aspect identified, the dissection continues anteriorly and laterally toward the sciatic nerve (Fig. 6). A careful release of any soft tissue bands is performed in a proximal to distal direction in order to mobilize the nerve and protect it throughout the procedure. This is especially important in cases of acute avulsions, where the nerve may be more difficult to identify secondary to hematoma, early adhesions, or tethering by the retracted tendons. The posterior femoral cutaneous nerve is often the first branch of the nerve identified during dissection and serves as a harbinger of the main sciatic nerve.

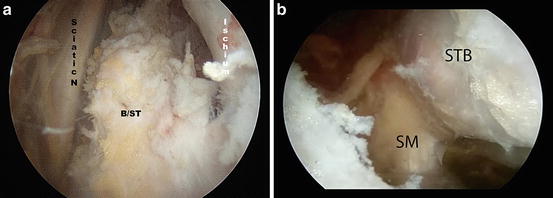
Fig. 5
In the prone position, the standard portals for endoscopic hamstring repair include a medial and lateral portal that are about 2 cm on either side of the palpable ischium. A third portal can be established about 4 cm distal to the tip of the ischium. The arthroscope is in the medial portal and the cautery is in the lateral portal
Fig. 6
Endoscopic views of the subgluteal space in a left hip. The arthroscope is in the lateral portal. (a) The sciatic nerve (SN) has been exposed along with biceps and semitendinosus avulsion (BST) and the lateral ischium (I). (b) The separate attachments of the semimembranosus (SM) tendon, which is more anterior and medial, and the common biceps and semitendinosus (BST) tendon more posterior and lateral
With the nerve identified and protected, the tendinous origin is then inspected for any obvious tearing (Fig. 7). In acute tears, the tear is obvious and the tendon is often retracted distally. In these cases, there may be a large hematoma that requires evacuation.
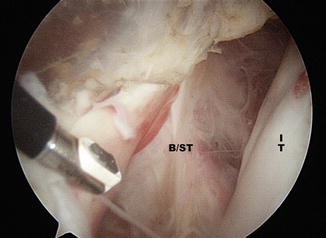
Fig. 7
 Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum




Endoscopic view of a proximal hamstring origin avulsion in a left hip with the arthroscope in the lateral portal. The distal end of the ischium is seen with fibrous tissue attachment (IT) and the avulsed ischial origin of the common tendon is seen to the left (B/ST)
Related posts:
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
