Fig. 1
X-ray of a patient that was shot in the buttock region. A previous surgeon attempted a bullet removal from an open posterior approach. This was unsuccessful. The bullet appears to be through the articular surface
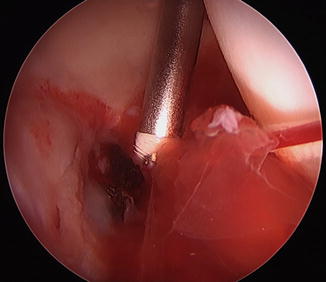
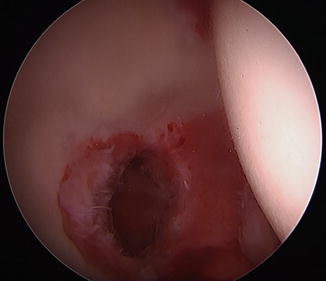
Fig. 2
Arthroscopic images of the same bullet in Fig. 1. The anatomy of the hip often obscures the true location of the fragment. This bullet was removed arthroscopically
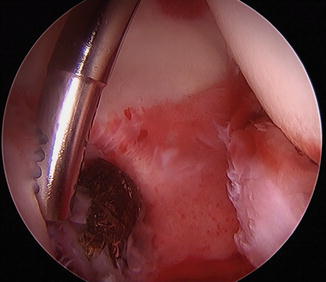
Fig. 3
A shaver is used to free the bullet from its resting place in the acetabular cartilage
Once the location and pathology have been defined, appropriate equipment is necessary. A standard arthroscopic grasper will not be able to retrieve a bullet. The two graspers mentioned above are excellent options (Fig. 4). Additional equipment that may be useful include threaded Steinmann pins that as described by Lee et al. [4] can be used to drive the threaded end into the soft bullet for control.
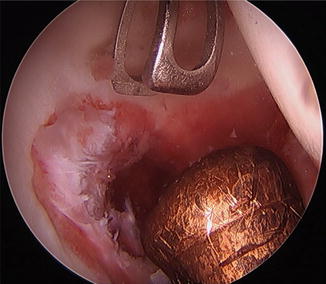
Fig. 4
Arthrex AR-16400 grasper used to remove the bullet from the hip joint
During supine hip arthroscopy, the bullet will most frequently remain in the posteroinferior aspect of the joint. This can make access from the anterior portal difficult. In these cases, a posterolateral portal should be established. This portal is created under spinal needle localization at the posterosuperior aspect of the greater trochanter. A switching stick or second grasper can then be used to “lever” the bullet out from the posterior aspect of the joint (Figs. 5 and 6) and support it while the grasper is used from the anterior portal to remove the fragment (Fig. 7). The anterior capsulotomy and portal will need to be large enough to support the bullet, and traction can be increased to allow the bullet to pass through the joint (Figs. 8 and 9).


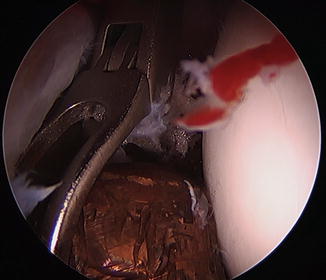
Fig. 5
A posterolateral portal is established and a second grasper is used to bring the bullet fragment more anterior and accessible
Fig. 6
The bullet is then brought into the anterior aspect of the joint where it is more accessible for removal
Fig. 7
A large grasper is used through the anterior portal to remove the bullet
Fig. 8
Distraction is increased across the hip joint in order to accommodate the size of the bullet
The Posterior Wall or Femoral Head Fragment After a Hip Dislocation
These are the most common and reported case of loose body removal. Various authors have reported a high percentage of retained fragments after these injuries. The technique required is dependent on the fragment size. Matsuda has even fixed a femoral head fracture arthroscopically with screws [11]. However, more commonly, only fragment removal is required. One of the more difficult aspects to these cases includes the establishment of appropriate visualization. An acute injury often disrupts the hip capsule and brings additional tissue into the joint. This can make maintenance of pressure difficult and visualization tricky. An early outflow portal can provide assistance, but often the tissue is thick and additional measures are required to establish a view. The senior author typically uses a curved shaver for hip arthroscopy, but in these cases a straight shaver can be very beneficial. An outflow spinal needle can be established blindly and confirmed by the outflow of fluid. A nitinol wire is then used to establish a full outflow cannula. This too is occasionally necessary to do blindly. Lastly, the straight shaver can be inserted through the cannula, directed away from the labrum and used on oscillate to remove this tissue. In the rare circumstance, the shaver can also be used blindly in the joint.
Related posts:
 Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


