Fig. 1
The patient is placed in the lateral decubitus position with posts or beanbag. Surgical prep should extend from above iliac crest and include entire operative extremity (Copyright Thomas J. Ellis)
Bony Landmarks
The greater trochanter should be palpated carefully to establish its anterior, posterior, and superior extent. This should be outlined with a marking pen. The iliac crest should be palpated and marked as well with particular note of the anterior superior iliac spine (ASIS) and anterior inferior iliac spine (AIIS). The latter will be only palpable in thin individuals.
Incision
A straight lateral skin incision is used. The length of the incision depends on the size of the patient but is typically 20–25 cm in length. The incision is centered over the anterior third of the greater trochanter and is oriented in a slightly proximal/posterior to distal/anterior direction.
Superficial Dissection
The skin and subcutaneous tissues are incised sharply. A Gibson or Kocher-Langenbeck approach may be used; however, the Gibson approach , which utilizes the interval between gluteus maximus and gluteus medius, lowers the risk of injury to the inferior gluteal nerve. The interval between gluteus maximus and medius can be identified by a number of small perforating vessels which are branches of the inferior gluteal artery typically run in this area. The overlying fascia is incised sharply to reveal the fibers of the two muscles. This fascial incision is carried longitudinally down over the trochanter and vastus lateralis to the inferior aspect of the operative field. As the fascia is opened, the insertion of the gluteus maximus tendon on the posterior aspect of the femur should be noted in the inferior aspect of the field.
Deep Dissection
At this point, internal rotation of the hip aids in visualization as the dissection progresses. Returning to the proximal portion of the field, close inspection of the gluteus medius reveals a thin fascial layer overlying this muscle which may be incised and elevated at its posterior aspect. Any bursal tissue should be excised from the greater trochanter. This will reveal the trochanteric branch which arises from the deep branch of the medial femoral circumflex artery running along the posterior aspect and up onto the lateral surface of the greater trochanter. Attention is turned to the posterior aspect of the gluteus medius near its trochanteric insertion. A strip of fatty tissue will be noted here, and the tissue should be carefully spread to reveal the piriformis tendon underneath running toward the piriformis fossa (Fig. 2). Care should be taken when dissecting as this area is quite vascular as it contains an anastomosis between the inferior gluteal artery and the deep branch of the medial circumflex artery.

Fig. 2
The piriformis tendon, running toward the piriformis fossa, is revealed. This region is highly vascular and care must be taken during dissection (Copyright Thomas J. Ellis)
Trochanteric Osteotomy
The hip is further internally rotated to bring the posterior aspect of the trochanter into full view in the center of the field. In preparation for the osteotomy, electrocautery can be used to mark the path of the osteotomy along the posterior aspect of the greater trochanter (Fig. 3). Vessels running along the posterior trochanter can be coagulated as well. The osteotomy should be made such that the majority of the gluteus medius insertion and vastus lateralis origin remain attached to the trochanteric fragment. The hip is internally rotated, and the blade of the sagittal saw should be roughly parallel to the leg to maintain the proper trajectory for the osteotomy as it progresses from posterior to anterior across the greater trochanter from the posterior superior trochanter toward the vastus ridge (Fig. 4). A finger may be placed over the top of the piriformis tendon during the cut to ensure that this critical area is not violated by the saw blade. The piriformis tendon and other short external rotators should remain attached to the femur to protect the vascular supply to the femoral head via the deep branch of the medial femoral circumflex artery (MFCA). This vessel travels proximal to the quadratus femoris, crosses the obturator externus, and continues anterior to the superior and inferior gemellus and obturator internus.

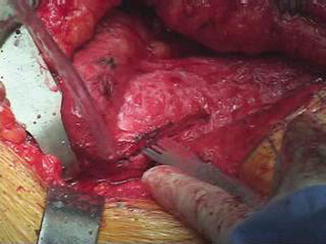
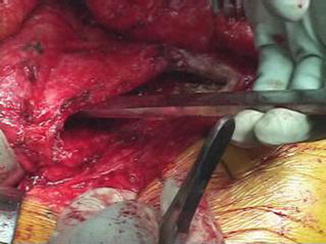
Fig. 3
Posterior aspect of the greater trochanter. Electrocautery is used to mark the osteotomy path (Copyright Thomas J. Ellis)
Fig. 4
The osteotomy progresses posterior to anterior across the greater trochanter toward the vastus ridge (Copyright Thomas J. Ellis)
The majority of the trochanteric osteotomy can be accomplished with the sagittal saw; however, it is advisable to leave the anterior cortex of the trochanter intact and to finish this part with an osteotome (Fig. 5). This leaves an anterior cortical ridge which may increase stability of the trochanteric fragment for later refixation. Next, a broad osteotome is used to carefully lever the trochanter anteriorly completing the osteotomy. At the distal aspect, the vastus lateralis fibers are carefully elevated off of the femur with either scalpel or electrocautery. Proximally the remaining posterior fibers of gluteus medius are incised sharply from the trochanteric remnant (Fig. 6). In order to protect the MFCA, identify the piriformis tendon and keep the knife blade between the medius tendon fibers and the piriformis tendon. It is advisable to avoid electrocautery in this area due to the close proximity to the medial circumflex artery. Identify the interval between the gluteus minimums and piriformis. The inferior margin of the gluteus minimus often lies underneath the piriformis muscle. This should allow for a blunt, curved Hohmann-type retractor to be slid from posterior to anterior into the interval and be positioned along the lateral and anterior joint capsule. Care should be taken to avoid damaging the minimus muscle belly during this maneuver. Flexing and externally rotating the hip will aid in anterior retraction of the medius, minimus, and trochanteric fragment. Placement of a pointed Hohmann-type retractor along the anterior aspect of the femur at the level of the osteotomy will also aid in flipping the trochanteric fragment anteriorly. Using cautery or sharp dissection, release remaining fascial attachments of the minimus muscle from the intact trochanter to expose the joint capsule. Flexing and externally rotating the leg will “open up” the anterior joint and facilitate this portion of the exposure. A self retaining Charnley-type retractor can be placed between the gluteus maximus and the trochanteric fragment to maintain capsular exposure.
 Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum




Related posts:
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
