Fig. 12.1
Arthroscopic repair of SLAP lesion. (a) Standard posterior viewing portal demonstrating SLAP tear. (b) Mobilized labrum following debridement. The superior glenoid surface is also prepared using an arthroscopic rasp. (c) SLAP repair performed using a knotless technique with 2.9 mm Pushlock anchors (Arthrex Inc, Naples, FL)
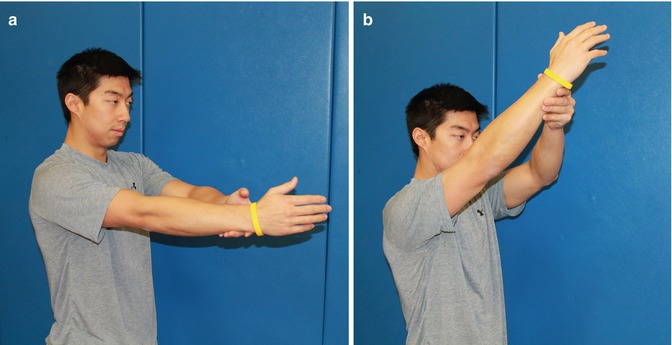
Fig. 12.2
(a, b) Active assisted forward flexion to 145°
A Neviaser portal is established under direct visualization using a spinal needle followed by a #1 Prolene (Ethicon, New Brunswick, NJ, USA) stitch. We then shuttle a # 2 Fiberwire (Arthrex, Naples, Florida, USA) and create a luggage tag stitch.
While the anchor and suture configuration is individualized based on the tear pattern, the authors prefer a knotless technique. We drill a pilot hole for a 2.9 Pushlock (Arthrex, Naples, Florida, USA) inserted at the 12 o’clock position. We then switch the arthroscope to the anterolateral portal to create a small accessory posterolateral portal with a 4 mm cannula. The aforementioned steps are then repeated to complete placement of a 2.9 Pushlock anchor at the 2 o’clock position (Fig. 12.3).
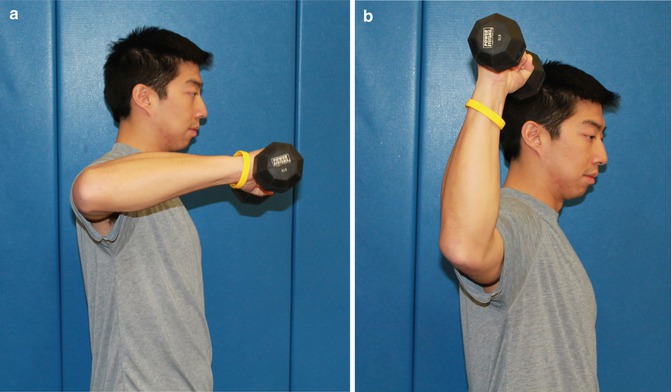
Fig. 12.3
(a, b) Rotator cuff strengthening with external rotation in 90° of abduction
The repair site is then tested with traction applied to the biceps tendon with an arthroscopic probe to ensure attachment of the labrum. This is followed by confirmation of a negative peel-back sign with the arm in abduction and external rotation. Associated injuries are then addressed on an individual patient basis.
12.7 Rehabilitation
Progression through each rehabilitation phase is both criteria-based and patient-specific. Phases and time frames are designed to give the clinician a general sense of progression.
12.7.1 Postoperative Phase I (Weeks 0–4)
12.7.1.1 Objectives
Promote healing: reduce pain and inflammation
Elevation in plane of scapula to 90°
External rotation: surgeon directed
Independent home exercise program provided
12.7.1.2 Safeguard
Immobilizer at all times, except when exercising or bathing
External rotation and extension limited to neutral
12.7.1.3 Evaluation and Treatment
Gripping exercises while in immobilizer
Active assisted range of motion from external rotation to neutral in the plane of the scapula
Active range of motion of the wrist/elbow (supported to avoid biceps stress)
Scapular mobility and stability (side-lying, progressing to manual resistance) pain-free
12.7.1.4 Minimum Criteria for Advancement to Phase II
External rotation: at least to neutral (surgeon directed)
Elevation in plane of scapula to 90°
Minimal pain or inflammation
12.7.2 Postoperative Phase II (Weeks 4–8)
12.7.2.1 Objectives
Continue to promote healing
Active assisted forward flexion to 145° (Fig. 12.2a, b)
External rotation to 60°
Begin to restore scapula and upper extremity strength
Restore normal scapulohumeral rhythm
12.7.2.2 Safeguard
Limited external rotation to 30° until 6 weeks.
Avoid excessive stretch to the labrum and biceps.
Avoid rotator cuff inflammation.
12.7.2.3 Evaluation and Treatment
Discontinue immobilizer (surgeon directed).
Continue active assisted range of motion elevation in the plane of the scapula with external rotation limited to 30° until 6 weeks.
Isometric internal/external rotation (submaximal and pain-free) progressing to isotonic internal/external rotation strengthening at 6 weeks.
Begin humeral head stabilization exercises such as scapular plane elevation with emphasis on scapulohumeral rhythm.
Begin latissimus strengthening, limited to 90° forward flexion.
12.7.2.4 Minimum Criteria for Advancement to Phase 3
Elevation in plane of scapula to 145°
External rotation to 60°
Internal rotation/external rotation strength 5/5
Normal scapulohumeral rhythm with minimal pain and inflammation
12.7.3 Postoperative Phase III (Week 8–14)
12.7.3.1 Objectives
Restore full shoulder range of motion
Restore normal scapulohumeral rhythm
Isokinetic internal/external strength 85 % of uninvolved side
Restore normal flexibility
12.7.3.2 Safeguard
Avoid rotator cuff inflammation.
Avoid excessive passive stretching.
12.7.3.3 Evaluation and Treatment
Aggressive scapular strengthening. Begin latissimus and biceps strengthening.
Progress internal/external rotation to 90/90 position (Fig. 12.3a, b).
12.7.3.4 Minimum Criteria for Advancement
Normal scapulohumeral rhythm
Minimal pain and inflammation
Full upper extremity range of motion
Isokinetic internal/external rotation strength 85 % of uninvolved side
12.7.4 Postoperative Phase IV (Weeks 14–18)
12.7.4.1 Emphasize
Monitoring symptoms
12.7.4.2 Objective
Restore normal neuromuscular function
Maintain strength and flexibility
Isokinetic internal/external strength equal to the unaffected side
12.7.4.3 Safeguard
Pain-free plyometricsRelated posts:
 Treatment of Unstable Simple Elbow Dislocations
Treatment of Unstable Simple Elbow Dislocations
 Posterosuperior and Anterosuperior Impingement in Overhead Athletes
Posterosuperior and Anterosuperior Impingement in Overhead Athletes
 Biomechanics of the Shoulder: Stability and Kinematics of Shoulder Motion, Throwing Kinematics
Biomechanics of the Shoulder: Stability and Kinematics of Shoulder Motion, Throwing Kinematics
 Biceps Instability: With Versus Without Rotator Cuff Lesions
Biceps Instability: With Versus Without Rotator Cuff Lesions
 Rehabilitation: Part I. Basic
Rehabilitation: Part I. Basic
 Rehabilitation: Part II. Advanced
Rehabilitation: Part II. Advanced

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


