Pattern
Definitions
Type 1
The prominence of the inferior medial scapular angle. It would be associated with excessive anterior tilting of the scapula
Type 2
The prominence of the entire medial border. It would be associated with excessive scapular internal rotation
Type 3
The prominence of the superior scapular border. It would be associated with excessive superior translation of the scapula
Type 4
It is normal, with no asymmetries identified and no prominence of the medial or superior border observed

Fig. 15.1
Scapular dyskinesis. (a) Type 1 dyskinesis, with inferior medial border prominence (both scapulae, but left is more definite.). (b) Type 2 dyskinesis, with prominence of the entire medial border (both scapulae, but left is more definite). (c) Type 3 dyskinesis, with prominence of the superior medial border (left scapula). (d) Type 4 dyskinesis, with normal scapular motion and position (both scapulae)
15.3 Assessment of Scapular Dyskinesis Using 3-D Wing CT
There are two studies using 3-D wing CT in assessing scapular dyskinesis. In these studies, the 3-D wing CT images were acquired using a 16- or 64-slice multidetector CT (MDCT) scanner (LightSpeed Pro16 or LightSpeed VCT, GE Healthcare, Little Chalfont, Bucks, UK). Each subject was examined in a supine position or prone position with the arms at the side of the body and the palms toward the body. The 3-D wing CT images depicted the thoracic region, consisting of bilateral scapula, bilateral clavicle, and the spine from the C7 to T7 vertebra [3, 4].
15.3.1 Five Motions of Scapula and Measurement of Five Angles of Scapular Position in 3-D Wing CT
15.3.1.1 Five Motions of Scapula
Scapular movement is a composite of three motions – upward/downward rotation around a horizontal axis perpendicular to the plane of the scapula, internal/external rotation around a vertical axis through the plane of the scapula, and anterior/posterior tilt around a horizontal axis in the plane of the scapula. The clavicle acts as a strut for the shoulder complex, connecting the scapula to the central portion of the body. This allows two translations to occur – upward/downward translation on the thoracic wall and retraction/protraction around the rounded thorax [18–20] (Fig. 15.2).
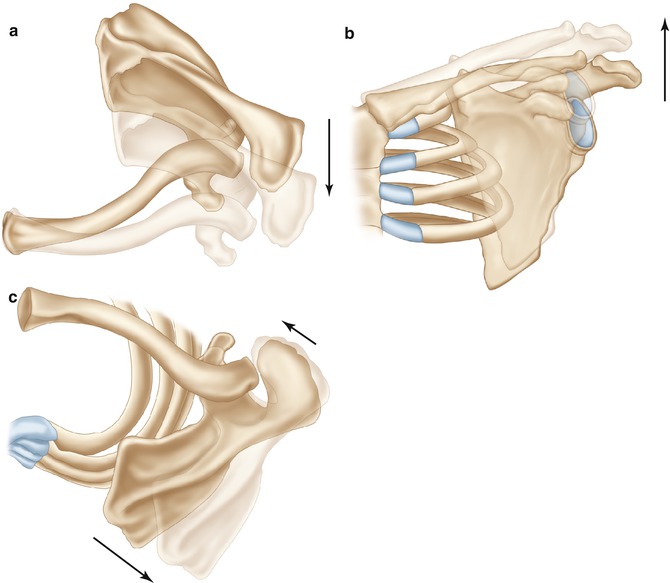
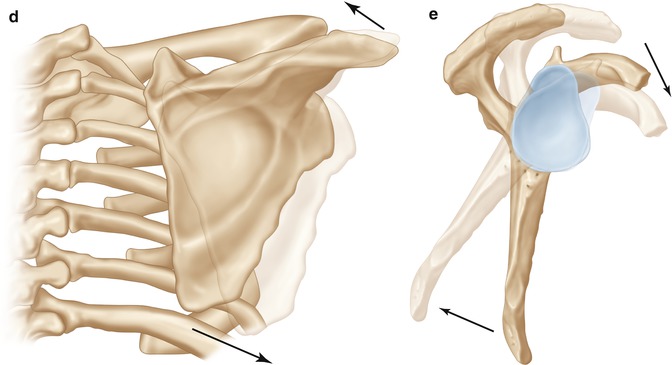
Fig. 15.2
Motions of the scapula. (a) Protraction. (b) Superior translation. (c) Internal rotation. (d) Upward rotation. (e) Anterior tilting
We adopted upward rotation (UR), superior translation (ST), anterior tilting (AT), protraction (PRO), and internal rotation (IR) as the representative five motions of scapula for simplification. Upward rotation is outward movement of inferior angle of the scapula as the arm is elevated. Superior translation is superior migration of the scapula with no medial or lateral movement. Anterior tilting of the scapula means that the acromion moves anteriorly and the inferior angle of the scapula moves posteriorly. Protraction is lateral translation of the medial border of the scapula without superior movement or rotation. Internal rotation means that the scapula rotates internally around a vertical axis. These are the three rotational movements and two translations of the scapula [3, 4, 18–20].
15.3.1.2 Measurement of Five Angles of Scapular Position in 3-D Wing CT
Because the acromioclavicular (AC) joint undergoes no translational movement during scapular rotation, the three bony landmarks defined were the inferomedial angle (IMA) of the scapula, the AC joint, and the root of the scapular spine (RSS). The measurement criteria included five movements of the scapula, consisting of three rotations and two translations: upward rotation, internal rotation, anterior tilting, superior translation, and protraction. Angular denominations were chosen for measurements to avoid false impressions due to anatomic variations, such as scapular size, scoliosis, and different acromion shapes [3, 4].
To avoid discrepancies in the measurement criteria, the midpoint of the AC joint was designated as the AC joint, the most caudal point of scapula as the IMA, and the most medial point of the scapular spine as the RSS. The five angles of scapular movement were measured, as below, with reference from several previous reports. There were a few modifications in measuring angles of scapula because of the 3-D wing CT setting [3, 4].
UR Angle
The UR angle is measured as the angle between the extension of line from the AC joint to RSS and the vertebral axis (C7–T7) on a posterior-coronal view [3, 4, 17, 18, 21] (Fig. 15.3a).
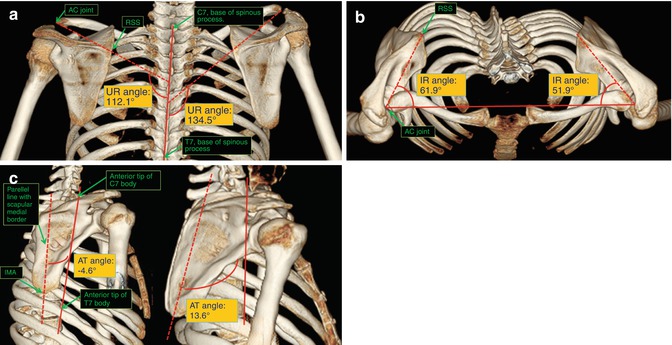
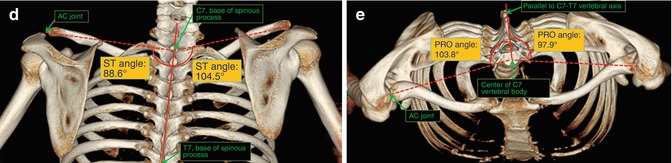
Fig. 15.3
The measurement of 5 angles on 3-D wing CT. (a) Upward rotation. (b) Internal rotation. (c) Anterior tilting. (d) Superior translation. (e) Protraction (Park et al. [4]). AC joint acromioclavicular joint, IMA inferomedial angle, RSS root of scapular spine
IR Angle
AT Angle
ST Angle
15.3.2 Statistical Analysis of Correlation Between the Five Angles of Scapular Position on 3-D Wing CT and the Observational Types of Scapular Dyskinesis
There are two studies about assessment of scapular dyskinesis using 3-D wing CT. In an earlier study of them, 89 athletes (178 shoulders) were videotaped and 7 blinded observers categorized scapular dyskinesis into 4 types, which was followed by 3-D wing CT in supine position. Four blinded examiners evaluated five angles [UR, IR, AT, ST, and PRO angles]. The inter-rater reliability (IRR) with observational assessment of scapular dyskinesis was good. The 3-D wing CT analysis had a very high IRR. There was a statistically significant correlation between observational assessment and 3-D wing CT analysis. The UR angle as well as the ST angle in type 3 scapular dyskinesis and the AT angle in type 1 scapular dyskinesis were increased as compared with those in the other types of scapular dyskinesis, and the difference was statistically significant. The IR angle in type 2 scapular dyskinesis was increased as compared with that in normal scapular motion, and the difference was statistically significant. The PRO angle in type 1 scapular dyskinesis was increased as compared with that in normal scapular motion, and the difference was also statistically significant [3].
In a more recent study of them, the 330 scapular movements of 165 patients were classified into 4 types by 7 blinded observers. Then, 3-D wing CT was performed with patients prone, and four blinded observers measured the above five angles [4]. UR and ST angles were significantly larger in type 3 more than in the other types, and the AT angle showed a similar pattern in type 1. The PRO angle was significantly larger in types 1, 2, and 3 more than in type 4, and the IR angle was significantly larger in type 2 more than in the other types [4]. The CT measurement in the more recent study showed a similar pattern with the previous study, but with some differences. First, the IR angle in type 2 increased significantly compared with those in other types, whereas the UR angle and ST in type 3 and the AT angle in type 1 are similar to our previous study. Second, the PRO angle increased significantly in types 1, 2, and 3 compared with that in type 4, whereas the IR angle increased only in type 1 in our previous study. Third, the cutoff values were determined for each angle to classify scapular dyskinesis according to the five angles. Fourth, the correlation among the classification according to the five angles and concomitant diseases was analyzed statistically [3, 4].
15.3.3 Cutoff Values of the Five Angles of Scapula in 3-D Wing CT in Prone Position According to a Significant Correlation with Each Observational Type
The cutoff values were determined for each angle among the types showing significant differences using the ROC curve (Table 15.2). The cutoff values of the five angles were UR, 117°; ST, 90°; AT, 8°; PRO, 99°; and IR, 51° [4].
Angle | Group vs. group | Cutoff value by ROC curve ° | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|
UR angle | Type 3 vs. types 1, 2, 4 | 117 | 84.6 | 74.1 |
ST angle | Type 3 vs. types 1, 2, 4 | 90 | 80.8 | 63.0 |
AT angle | Type 1 vs. types 2, 3, 4 | 8 | 94.6 | 84.5 |
PRO angle | Types 1, 2, 3 vs. type 4 | 99 | 70.0
Related posts: Treatment of Unstable Simple Elbow Dislocations Treatment of Unstable Simple Elbow Dislocations
 Rotator Cuff Tear in Athletes: Part III. Surgical Treatment Rotator Cuff Tear in Athletes: Part III. Surgical Treatment
 Biomechanics of the Shoulder: Stability and Kinematics of Shoulder Motion, Throwing Kinematics Biomechanics of the Shoulder: Stability and Kinematics of Shoulder Motion, Throwing Kinematics
 Biceps Instability: With Versus Without Rotator Cuff Lesions Biceps Instability: With Versus Without Rotator Cuff Lesions
 Rehabilitation: Part I. Basic Rehabilitation: Part I. Basic
 Rehabilitation: Part II. Advanced Rehabilitation: Part II. Advanced
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|