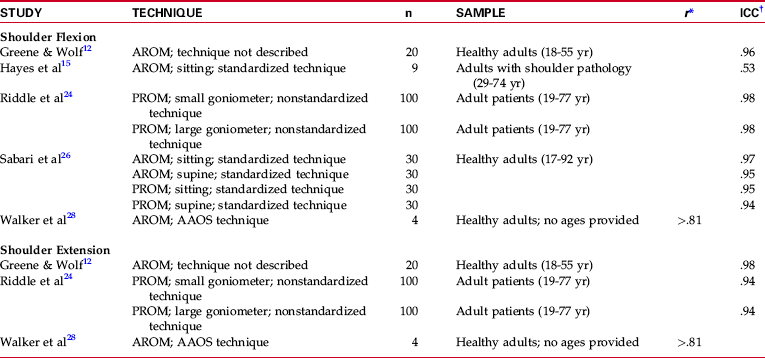
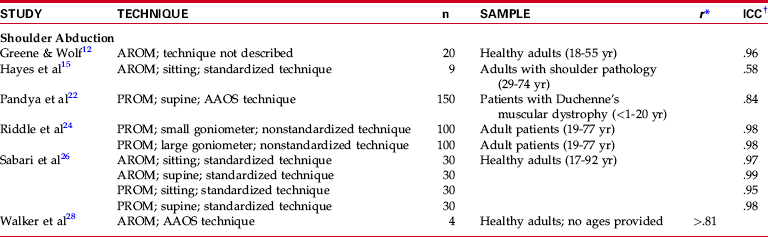
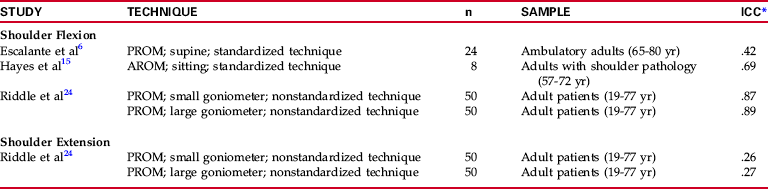
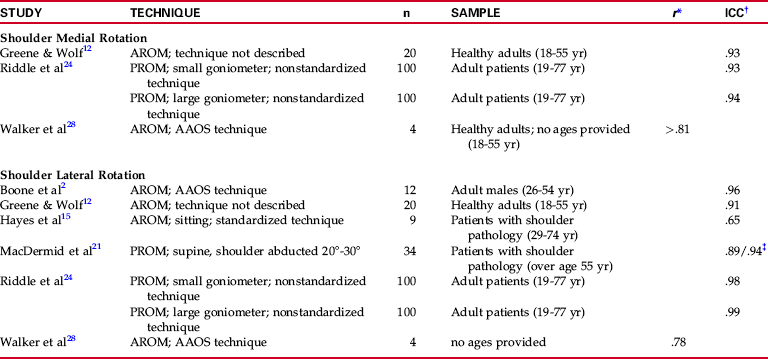
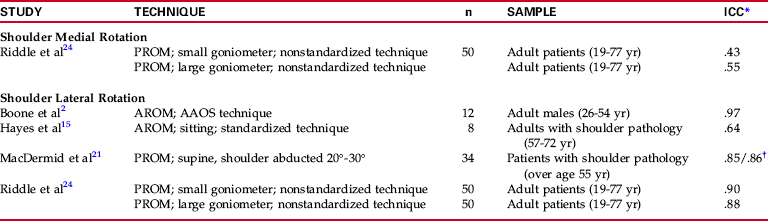
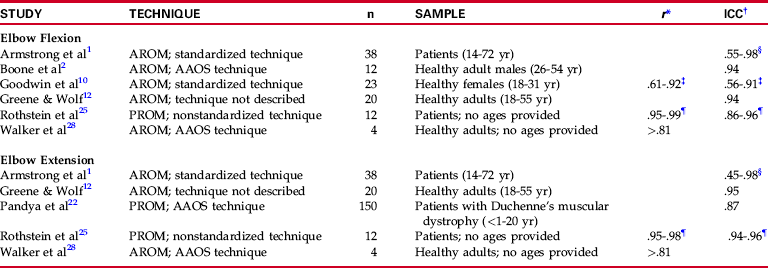
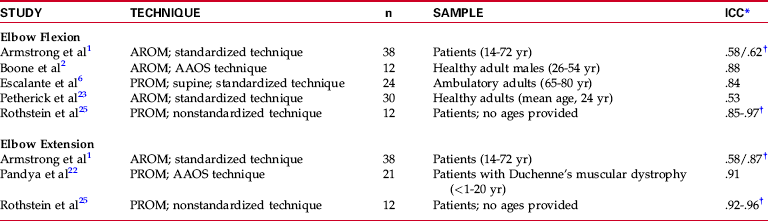
Chapter 7 Chapters 3 through 6 described techniques for measuring joint range of motion (ROM) and muscle length of the upper extremity. Research regarding the reliability and validity of joint ROM techniques, including the goniometer and the inclinometer, is presented in this chapter (no studies examining the reliability of upper extremity muscle length testing were found). Only those studies that provide information as to both relative and absolute reliability or validity are included. More detailed information regarding appropriate analysis of reliability and validity is presented in Chapter 2. A moderate amount of research has focused on the reliability of shoulder flexion and extension goniometry. The reliability of passive shoulder flexion and extension goniometry was studied by Riddle et al.24 This group of investigators examined both intrarater and inter-rater reliability of passive shoulder flexion and extension ROM in a group of 100 adult patients aged 19 to 77 years. The investigators used no standardized goniometric technique or patient positioning in this study. In an effort to determine whether the size of the goniometer used made a difference in the reliability obtained, two different sizes of universal goniometers were employed for the study. Intraclass correlation coefficients (ICCs) were calculated both within and between raters for each type of goniometer used. Intrarater reliability did not vary, and inter-rater reliability varied only slightly with the type of goniometer used to measure both shoulder flexion and extension. However, although intrarater reliabilities for shoulder flexion and extension were good (.98 for flexion and .94 for extension) (Table 7-1), inter-rater reliability for shoulder flexion was not as high (.87 and .89, respectively), and inter-rater reliability for shoulder extension was poor (.26 and .27, respectively) (Table 7-2). Table 7-2 Inter-Rater Reliability: Shoulder Flexion/Extension Range Of Motion AROM, Active range of motion; PROM, passive range of motion. Passive shoulder flexion was measured in 695 subjects as part of the San Antonio Longitudinal Study of Aging.6 Before initiating the study, the four examiners who measured ROM participated in a preliminary investigation to determine inter-rater reliability. Passive shoulder flexion was measured by each of the four examiners in 24 adults aged 65 to 80 years. Measurements were taken with the subjects positioned supine using a standardized measurement technique. Inter-rater reliability was analyzed using an ICC. Results indicated only fair reliability for the measurement of shoulder flexion (ICC = 0.42; see Table 7-2). A greater number of investigators have examined active shoulder flexion and extension goniometry than have examined passive flexion and extension goniometry. In a study designed to compare the reliability of the OrthoRanger (an electronic, computerized goniometer) and the universal goniometer, Greene and Wolf12 examined intrarater reliability of active shoulder flexion and extension goniometry, in addition to 12 other motions of the upper extremity, in 20 healthy adults. Measurements of shoulder flexion and extension each were taken three times per session across three testing sessions by the same examiner. Intrarater reliability for these measurements was analyzed using an ICC. Results revealed high reliability for the universal goniometer (.96 for flexion, .98 for extension) for both active shoulder flexion and extension (see Table 7-1). The 95% confidence interval (CI) for the universal goniometer was 3.9 degrees for shoulder flexion and 2.4 degrees for shoulder extension. Walker and colleagues28 also examined intrarater reliability of active shoulder flexion and extension goniometry. In a study designed to determine the normal active ROM of 26 movements of the upper and lower extremities in older adults, measurements were taken in 60 persons aged 60 to 84 years. Techniques recommended by the American Academy of Orthopaedic Surgeons (AAOS) were used for all measurements. Before data collection, intrarater reliability was determined using four subjects. Although the exact number of motions measured to determine reliability was unclear from the authors’ description of their methods, they reported Pearson product moment correlation coefficients (Pearson’s r) for intrarater reliability “above .81” for active shoulder flexion and extension measurements (see Table 7-1) and a mean error between repeated measures of 5 degrees. In a report published in 1998, a group of investigators performed a study designed to determine whether intrarater reliability of measurements of active and passive shoulder flexion and abduction changed when subjects were placed in a seated as compared with a supine position.26 Two measurements were taken of each motion in each position in 30 adult subjects, aged 17 to 92 years. Data were analyzed using ICCs, which ranged from .94 to .97 for intrarater reliability of shoulder flexion, regardless of the type of motion measured (active or passive) or of the patient’s position during the measurement (supine or sitting) (see Table 7-1). However, paired t tests between goniometric readings taken in trial 1 compared with trial 2 revealed a significant difference (p < .05) in measurements of passive shoulder flexion taken in a supine position. Only one study was found that included the investigation of inter-rater reliability of active shoulder flexion using a goniometer. In a study that examined a variety of methods of assessing shoulder ROM, Hayes and colleagues15 used two separate groups of subjects with shoulder pathology to determine intrarater and inter-rater reliability of active shoulder flexion, abduction, and external rotation measurements taken with a goniometer. Ten shoulders were measured in nine subjects (aged 29 to 74 years) for the intrarater reliability trial, and eight subjects (aged 57 to 72 years) were used to investigate inter-rater reliability. Measurements of shoulder flexion were taken with subjects seated on the edge of a treatment table and with the stationary arm of the goniometer aligned with “a vertical line in the coronal plane.”15 Subjects were asked to flex the shoulder and stop at the point of pain. A single examiner (an orthopaedic surgeon) performed measurements for the intrarater reliability study. Four examiners (an orthopaedic surgeon, a sports medicine resident, and two physical therapists) participated in the inter-rater reliability study, with each examiner measuring each subject using five different ROM measurement methods. Intraclass correlation coefficients and standard errors of the mean (SEMs) were calculated for both intrarater and inter-rater reliability trials. Intrarater reliability for shoulder flexion was fair to good (0.53; see Table 7-1), and inter-rater reliability was higher at 0.69 (see Table 7-2). Standard errors ranged from 17 degrees for a single rater to 25 degrees between raters (see Table 7-2), although the authors of this study did not address specific reasons for the lower reliability found in this study as compared with others.12,26,28 Several possibilities, including lack of trunk stabilization during ROM measurements and the possibility that pain patterns changed in subjects during the course of multiple measurements, are apparent. Intrarater reliability of active shoulder abduction has been examined by four groups of investigators whose studies have been described previously.12,15,26,28 Techniques recommended by the AAOS were used in the study by Walker et a1,28 and Hayes and colleagues15 used a standardized technique of their own design. The remaining two studies were not specific regarding the measuring techniques employed. Three studies12,26,28 were performed in healthy adult subjects, and one study15 used only subjects with shoulder pathology. Greene and Wolf,12 Sabari et al,26 and Hayes et al15 analyzed their data using ICCs and performed follow-up measures of concordance on the data. Sabari et al26 reported correlations ranging from .97 to .99 for active shoulder abduction goniometry, depending on the patient position used (Table 7-3). Paired t tests revealed no significant difference (p > .05) between measures of active shoulder abduction range of motion taken in the two trials, regardless of patient position. Greene and Wolf12 analyzed their data using the ICC and reported intrarater reliability of .96 (see Table 7-3) and a 95% confidence level of 6.4 degrees. Hayes et al15 reported lower intrarater reliability of .58 with a 95% confidence level of 46 degrees in their population of patients with shoulder pathology. In the same study described previously, Hayes et al15 also examined inter-rater reliability of active shoulder abduction. Data analysis revealed an ICC of .69 (Table 7-4) for agreement between the four raters in the study and a 95% CI of 42 degrees. Walker et al28 used Pearson’s r for data analysis and reported a correlation of greater than .81 (see Table 7-3) and a mean error of 5 degrees (±1 degrees). Both Sabari et al26 and Riddle et al24 investigated the reliability of passive shoulder abduction goniometry in adult subjects. These studies, which have been described elsewhere (see the Shoulder Flexion/Extension section), yielded ICCs for intrarater reliability of passive shoulder abduction measurements ranging from .95 to .98 (see Table 7-3).24,26 However, follow-up paired t tests between goniometric readings taken in trial 1 compared with trial 2 in the study by Sabari et al26 revealed a significant difference (p < .05) in the measurement of passive shoulder abduction taken with the subject in a sitting position. Riddle et al24 also analyzed inter-rater reliability of passive shoulder abduction in adult subjects and reported somewhat lower correlations of .84, using a small goniometer, to .87, using a large goniometer (see Table 7-4). Both intrarater and inter-rater reliabilities have been reported for passive shoulder abduction measurements in children. Pandya et al22 examined intrarater reliability of passive shoulder abduction goniometry in 150 children with Duchenne’s muscular dystrophy.22 Intraclass correlation coefficients were used to analyze the data, and reliability was reported as .84 (see Table 7-3). Inter-rater reliability of passive shoulder abduction in a subgroup of 21 children with Duchenne’s muscular dystrophy also was examined, and reliability of .67 was reported (see Table 7-4). Reliability of passive shoulder rotation goniometry has been studied by only two groups of investigators. Riddle et al24 examined both intrarater and inter-rater reliability of measurements of passive shoulder ROM, including shoulder medial and lateral rotation, using two different sizes of universal goniometers. Range of motion was measured in 100 patients aged 19 to 77 years without the use of standardized measuring or positioning techniques. Intrarater reliability (ICC) for passive shoulder rotation ranged from .93, for medial rotation using a small goniometer, to .99, for lateral rotation using a large goniometer (Table 7-5). Reliability between raters for lateral rotation remained high and was reported as .90 and .88 for a small and a large goniometer, respectively. However, inter-rater reliability for passive shoulder medial rotation was fairly low, equaling .43 with a small goniometer and .55 with a large goniometer (Table 7-6). Table 7-5 Intrarater Reliability: Shoulder Medial/Lateral Rotation Range of Motion †Intraclass correlation coefficient. Table 7-6 Inter-Rater Reliability: Shoulder Medial/Lateral Rotation Range of Motion *Intraclass correlation coefficient. MacDermid et al21 also examined reliability of passive shoulder rotation goniometry but focused exclusively on passive lateral rotation measurements. In a study of 34 patients older than 55 years with shoulder pathology, MacDermid and colleagues21 measured passive lateral rotation of the shoulder while the patient was supine with the shoulder abducted 20 to 30 degrees. Both intrarater and inter-rater reliabilities were calculated using ICCs. Intrarater reliability was reported as .89 and .94 (see Table 7-5), and the standard error of measurement (SEMm) was 7.0 degrees and 4.9 degrees, varying according to the examiner who performed the measurement. Inter-rater reliability was .85 and .86 (see Table 7-6) with the SEMm reported as 7.5 degrees and 8.0 degrees, depending on whether the first or second measurement was used in the calculation. More groups have examined active shoulder rotation goniometry than have examined passive rotation goniometry. Greene and Wolf12 and Walker et a1,28 whose studies were described previously, investigated the intrarater reliability of goniometric measurements of active shoulder medial and lateral rotation. The study by Walker et al28 included four healthy adults and reported reliability of greater than .81 for shoulder medial rotation and .78 for lateral rotation (Pearson’s r) and a mean error of 5 degrees, whereas Greene and Wolf12 examined 20 healthy adults and reported a reliability of .91 (ICC) (see Table 7-5) and a 95% confidence level of 14.9 degrees for medial and 17.2 degrees for shoulder lateral rotation. The reliability of goniometric measurements of active shoulder lateral rotation was examined by Boone and colleagues2 in a group of 12 adult males aged 26 to 54 years. Four different examiners with varied experience in goniometry performed the measurements using AAOS measurement techniques. Measurements were taken once per week for 4 weeks by each of the four examiners. Average intrarater reliability was .96 (see Table 7-5), and repeated measures analysis of variance (ANOVA) revealed no significant intratester variation for measurements of shoulder lateral rotation. However, although average inter-rater reliability was .97 (see Table 7-6), repeated measures ANOVA demonstrated significant differences between two of the four examiners for measurements of shoulder lateral rotation. In a study described previously (see Active Shoulder Flexion/Extension), Hayes et al15 examined both intrarater and inter-rater reliability of active shoulder lateral rotation goniometry. Measurements were taken in two separate groups of patients with symptomatic shoulder pathology. Lateral rotation measurements were taken with the shoulder positioned at 0 degrees of abduction. Investigators reported an ICC of .65 for intrarater reliability (see Table 7-5) and .64 for inter-rater reliability (see Table 7-6). Ninety-five percent CIs in both instances were 28 degrees. Armstrong and colleagues1 examined intrarater and inter-rater reliability of active elbow and forearm goniometric measurements in a group of 38 patients aged 14 to 72 years. Each of the subjects had undergone a surgical procedure for an injury to the elbow, the forearm, or the wrist at a minimum of 6 months before measurement. Standardized measuring techniques and patient positioning were used during testing, in which three different instruments were employed to assess ROM. Instruments used for the study included a universal goniometer, a computerized goniometer, and “a mechanical rotation measuring device.” Only the universal goniometer and the computerized goniometer were used to measure elbow flexion and extension, as the rotation measuring device was capable of measuring only forearm rotation. Active elbow flexion and extension ROM were measured twice for each instrument on all subjects. Five different examiners, who possessed varied amounts of experience in performing goniometry, measured the amount of elbow flexion and extension in each subject. Both intrarater and inter-rater reliability were analyzed using ICCs. Intrarater reliability for active elbow flexion using the universal goniometer ranged from .55 to .98, depending on which examiner performed the measurements (Table 7-7). Similar intrarater reliability levels were obtained for active elbow extension, ranging from .45 to .98 (see Table 7-7). Of interest is the fact that the lowest reliability levels were produced by an experienced hand therapist, and less experienced examiners demonstrated higher reliability. Ninety-five percent CIs within raters averaged 6 degrees for elbow flexion and 7 degrees for elbow extension. Inter-rater reliability for elbow flexion using the universal goniometer was reported as .58 and .62, depending on which set of measurements was used for the analysis. Levels of inter-rater reliability reported by Armstrong et al1 were similar to levels of reliability reported previously by Petherick et al23 but were lower than the reliability reported by Boone et al2 (discussed subsequently). Elbow extension inter-rater reliability using the universal goniometer was reported as .58 and .87 (Table 7-8), again varying according to which set of measurements was used for the analysis. Ninety-five percent CIs between raters averaged 10 degrees for both elbow flexion and extension. Table 7-7 Intrarater Reliability: Elbow Flexion/Extension Range Of Motion †Intraclass correlation coefficient. Table 7-8 Inter-Rater Reliability: Elbow Flexion/Extension Range Of Motion *Intraclass correlation coefficient.
RELIABILITY and VALIDITY of MEASUREMENTS of RANGE of MOTION and MUSCLE LENGTH TESTING of the UPPER EXTREMITY
RELIABILITY AND VALIDITY OF UPPER EXTREMITY GONIOMETRY
Passive
Active
Shoulder Abduction
Passive
Shoulder Medial/Lateral Rotation
Active
Elbow Flexion/Extension
Related posts:
 MEASUREMENT of RANGE of MOTION and MUSCLE LENGTH: CLINICAL RELEVANCE
MEASUREMENT of RANGE of MOTION of the KNEE
MEASUREMENT of RANGE of MOTION and MUSCLE LENGTH: BACKGROUND, HISTORY, and BASIC PRINCIPLES
MEASUREMENT of RANGE of MOTION of the HIP
MEASUREMENT of RANGE of MOTION of the ANKLE and FOOT
PEDIATRIC RANGE of MOTION
MEASUREMENT of RANGE of MOTION and MUSCLE LENGTH: CLINICAL RELEVANCE
MEASUREMENT of RANGE of MOTION of the KNEE
MEASUREMENT of RANGE of MOTION and MUSCLE LENGTH: BACKGROUND, HISTORY, and BASIC PRINCIPLES
MEASUREMENT of RANGE of MOTION of the HIP
MEASUREMENT of RANGE of MOTION of the ANKLE and FOOT
PEDIATRIC RANGE of MOTION
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


RELIABILITY and VALIDITY of MEASUREMENTS of RANGE of MOTION and MUSCLE LENGTH TESTING of the UPPER EXTREMITY