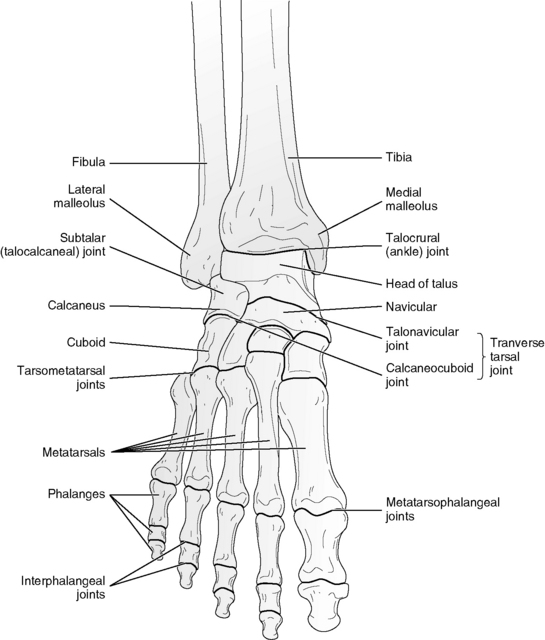
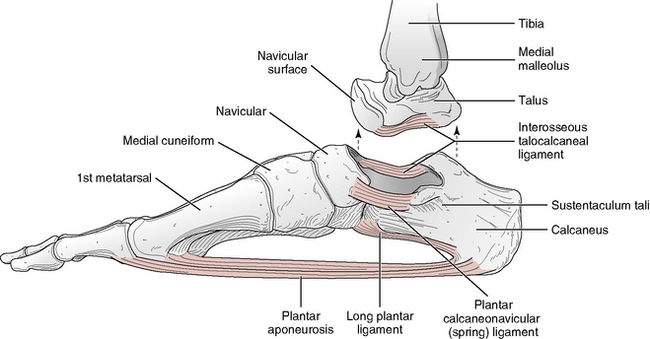
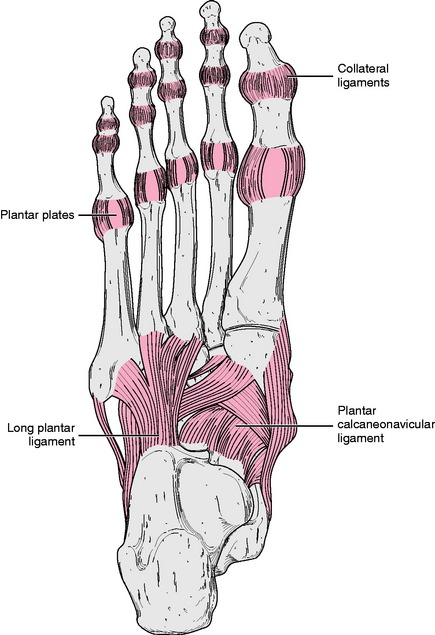
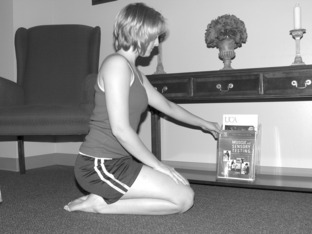
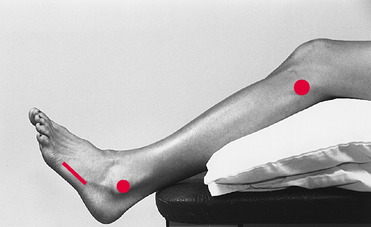
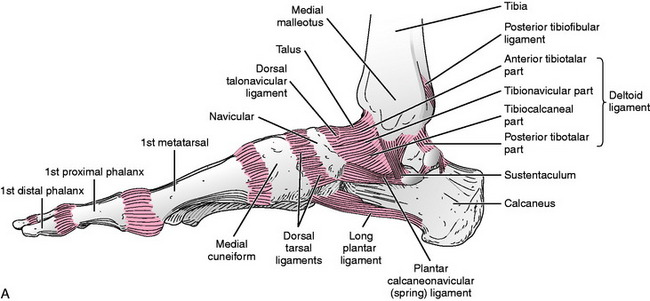
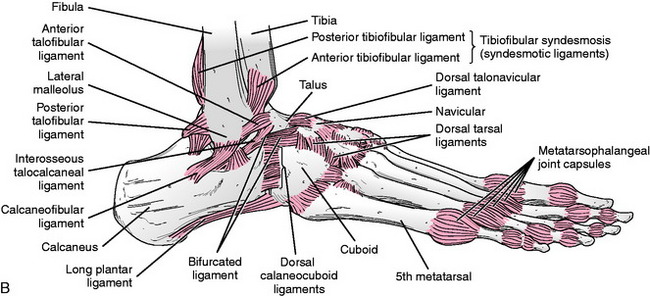
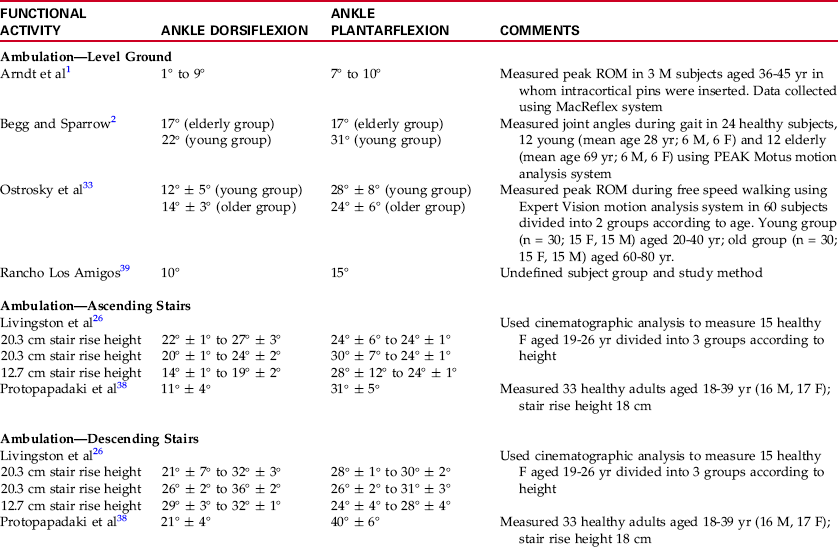
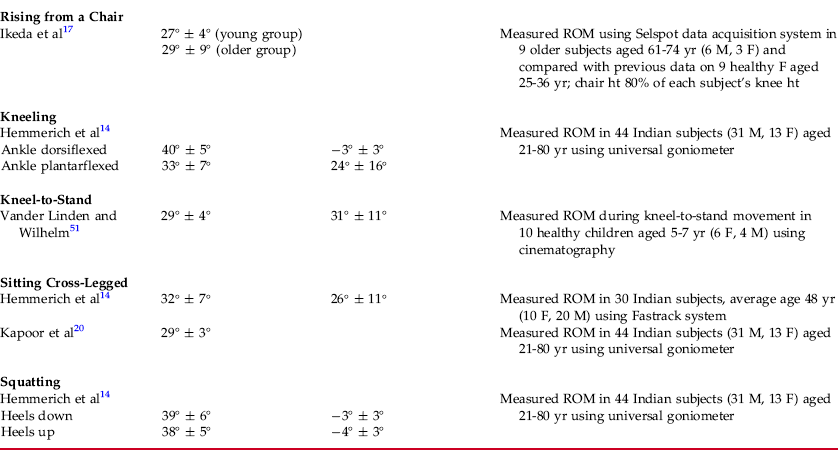
Chapter 13 The ankle, or talocrural, joint consists of the articulation of a concave proximal, mortise-shaped joint surface formed by the distal tibia and fibular malleolus, with the convex proximal surface of the talus (Fig. 13-1).5,7,24,31 Ligamentous reinforcement of the talocrural joint is provided by collateral ligaments that span the medial and lateral aspects of the joint. The medial collateral ligament, also termed the deltoid ligament, originates from the medial malleolus and spreads in a fan-shaped manner over the medial aspect of the ankle to attach to the talus, calcaneus, and navicular bones (Fig. 13-2, A).24,31 This ligament consists of superficial and deep bands and provides strong reinforcement to the medial side of the joint.35 The lateral collateral ligament of the ankle consists of three distinct components. From anterior to posterior, these include the anterior talofibular ligament, the calcaneofibular ligament, and the posterior talofibular ligament (Fig. 13-2, B). All three of these ligaments have their origin on the lateral malleolus. The two talofibular ligaments attach to the anterior and posterior aspects of the talus, and the calcaneofibular ligament has its inferior attachment on the calcaneus.5,31 Fig. 13-2 Ligaments of the ankle, subtalar, and transverse tarsal joints. A, Medial view. B, Lateral view. The subtalar, or talocalcaneal, joint is formed by two articulations—a posterior and an anterior—between the talus and the calcaneus (Fig. 13-3). The posterior articulation occurs between the convex posterior talar facet of the calcaneus and the concave posterior calcaneal facet of the talus. The anterior articulation, formed by contact between the convex head of the talus and the concave middle and anterior talar facets of the calcaneus, is also part of the talocalcaneonavicular joint (an articulation between the anterior aspects of the talus and the calcaneus and the posterior aspect of the navicular).7,21,40,46 A primary source of ligamentous stablility for the subtalar joint comes from two ligaments located within the sinus tarsi: the cervical ligament and the interosseous talocalcaneal ligament. Each of these ligaments is broad and strong and interconnects the talus superiorly with the calcaneus inferiorly.7,32,46 The subtalar joint receives additional reinforcement from the collateral ligaments of the ankle, as well as from anterior, posterior, and lateral talocalcaneal ligaments.7,22,32 The transverse tarsal joint is a collective term used for the combined talonavicular joint and the more laterally located calcaneocuboid joint (see Fig. 13-1). The talonavicular joint consists of the convex talar head articulating with a concave distal joint surface composed of the navicular bone and the spring ligament. Laterally, the joint surfaces of the transverse tarsal joint are irregular, as the distal surface of the calcaneus and the proximal surface of the cuboid are both convex and concave. Reinforcement of the transverse tarsal joint is provided via several ligaments that span its joints (see Fig. 13-2, A and B). The plantar calcaneonavicular, or spring, ligament supports the head of the talus by spanning the plantar surface of the talonavicular joint from the sustentaculum tali of the calcaneus to the navicular. More laterally, the plantar surface of the calcaneocuboid joint is supported by the long and short plantar ligaments, both of which originate from the plantar surface of the calcaneus and insert onto the metatarsal and cuboid bones. Dorsally, the transverse tarsal joint is reinforced by the dorsal talonavicular and calcaneocuboid ligaments and by the bifurcated ligament.7,31,32,43 Traditional anatomical descriptions of motion at the ankle (talocrural), subtalar, and transverse tarsal joints depict motions that occur at these joints as dorsiflexion, plantarflexion, inversion, and eversion in their classical definitions (see Chapter 1).7 However, more contemporary explanations describe motion at these joints as occurring around oblique axes that lie at angles to all three cardinal planes.10,25,32,42 These axes allow motion in all three planes simultaneously. The motions thus produced have been termed pronation (a combination of dorsiflexion, abduction, and eversion) and supination (a combination of plantarflexion, adduction, and inversion).10,22,32,42,50 However, much confusion surrounds these terms in the literature, with some authors using supination and pronation instead of, or interchangeably with, inversion and eversion.19,28,44 For purposes of this text, motion that occurs at the ankle, subtalar, and transverse tarsal joints is termed pronation and supination, with emphasis placed on the component motion of pronation or supination that is greatest at each joint. Motion at the ankle joint consists of pronation and supination around an oblique axis that angles, from lateral to medial, anteriorly and dorsally and passes through the talus and the tips of the medial and lateral malleoli.5,10,32 Movement around such an axis causes the major components of pronation and supination at the talocrural joint to be dorsiflexion and plantarflexion, respectively,28,32 which are the motions measured clinically to examine pronation and supination at this joint. Motion at the subtalar joint consists of pronation and supination around an oblique axis that extends, from lateral to medial, in an anterior and dorsal direction, falling through the head of the talus.29,36 Because of the location and angulation of the subtalar joint axis, the principal components of pronation and supination at this joint are eversion and inversion and abduction and adduction.25 Inversion and eversion are the motions that are measured clinically to examine supination and pronation of this joint.10 Although the talonavicular and calcaneocuboid joints do not share a joint capsule, their joint lines traverse the foot from medial to lateral in a roughly S shape, allowing motion to occur across the combined joints.7 The primary components of pronation and supination that occur at this joint add to the component motions of dorsiflexion/plantarflexion at the ankle and eversion/inversion at the subtalar joint. Because no adequate means of measuring isolated transverse tarsal motion is known, motion at this joint is measured in this text in conjunction with subtalar motion as foot inversion and eversion. During the dorsiflexion component of ankle pronation, the talus rolls anteriorly and slides posteriorly; the reverse movements occur during the plantarflexion component. Supination and pronation at the subtalar joint occur as a result of sliding of the calcaneus on the talus (open-chain motion) around an oblique axis. During pronation and supination at the transverse tarsal joint, spin occurs between the concave distal joint surface formed by the navicular and spring ligament and the convex talar head.32 The dorsiflexion and plantarflexion components of ankle pronation and supination are limited by the joint capsule, as well as by ligaments and muscles that cross the joint. Ankle plantarflexion is limited initially by tension in the muscles that dorsiflex the ankle and then by anterior capsular and ligamentous structures, including the anterior talofibular ligament and the tibionavicular fibers of the deltoid ligament.24,32 Ankle dorsiflexion is limited by tension in the soleus and gastrocnemius muscles, particularly if the knee is extended when the movement occurs. Posterior capsular and ligamentous structures, including the calcaneofibular ligament, the posterior talofibular ligament, and the tibiotalar fibers of the deltoid ligament, also limit ankle dorsiflexion, particularly with the knee flexed.24,32 Inversion and eversion of the subtalar and transverse tarsal joints are limited by tension in the lateral and medial collateral ligaments of the ankle, respectively.19,32 Information on normal ranges of motion for the dorsiflexion, plantarflexion, inversion, and eversion components of pronation and supination is found in Appendix B. The metatarsophalangeal (MTP) joints of the foot are similar in structure to the metacarpophalangeal joints of the hand.10,19 Each of the five MTP joints is formed by the articulation of the convex metatarsal head with the concave base of the proximal phalanx of the corresponding digit (see Fig. 13-1).7 A pair of collateral ligaments reinforces the sides of each MTP joint, and the plantar aspect of each joint is reinforced by the plantar plates (Fig. 13-4). These plantar plates, or ligaments, are composed of dense fibrous connective tissue, and all five are interconnected by the deep transverse metatarsal ligaments.7,32 The interphalangeal (IP) joints of the toes are classified as hinge joints, and each interphalangeal joint is composed of an articulation between the convex head of the more proximal phalanx and the concave base of the more distal phalanx (see Fig. 13-1). Nine such interphalangeal joints are found in the toes—two (one proximal and one distal) in each of the lateral four toes, and one interphalangeal joint in the great (first) toe. Ligamentous reinforcement of the interphalangeal joints is similar to that of the metatarsophalangeal joints, although the ligaments are smaller and the plantar plates are not interconnected (see Fig. 13-4).7,19,32 Motions at the metatarsophalangeal joints, as at the metacarpophalangeal joints, consist of flexion, extension, abduction, and adduction, although the range of abduction and adduction available in the toes is much less than that seen in the fingers, with active abduction and adduction of the first MTP joint being impossible for some individuals. Only the movements of flexion and extension are available at the interphalangeal joints of the toes. More motion is possible at the proximal interphalangeal joints than at the distal, and flexion is generally greater than extension at all joints.7,19,32 During flexion and extension at both the metatarsophalangeal and interphalangeal joints, the concave distal joint surface (base of the phalanx) rolls and slides on the convex proximal joint surface in the same direction as the external motion. For example, during MTP flexion, the base of the proximal phalanx rolls and slides in a plantar direction. The reverse motion occurs during MTP extension.32 MTP and IP joint flexion is limited by tension in the toe extensor muscles and tendons, whereas extension is limited by tension in the toe flexor muscles and tendons and the plantar ligaments. Abduction and adduction at the MTP joints are limited by the collateral ligaments of the joints or by approximation with adjacent toes.7,32 Information regarding the normal ranges of motion for the MTP joints is located in Appendix B. The capsular pattern varies in the metatarsophalangeal and interphalangeal (PIP and DIP) joints depending on which joints are involved. For the first (great) toe, the capsular pattern is one of extension that is more limited than flexion. For the second through fifth toes, capsular involvement is suspected when flexion is more limited than extension.8,18 Several investigators have examined the motion of the ankle joint during functional activities, particularly those related to ambulatory activities such as walking on level ground1,2,33,39 and ascending and descending stairs (Fig. 13-5).26,38 Additional investigations have examined ankle motion during other daily activities such as rising from a chair17 and transitioning from a kneeling to a standing position.51 A few authors also have examined ankle motion in so-called high range of motion (ROM) activities such as kneeling (Fig. 13-6), squatting, and sitting cross-legged.14,20 A summary of ankle range of motion related to various functional activities is located in Table 13-1. Most of the studies from which data were derived were performed in healthy adults, although some investigations included elderly and pediatric subjects. Essentials of the study populations and instrumentation used are included in the table. Caution should be used in extrapolating these data to the general population because the sample sizes for almost all of the studies were small. For more in-depth information on each study, the reader is referred to the reference list at the end of this chapter. Table 13-1 Ankle Rom Requirements for Functional Activities Expert Vision Motion Analysis System by Motion Analysis Corp, Santa Rosa, California. Selspot Data Acquisition System by Selective Electronic Company (SELCOM), Molndal, Sweden. Peak Motus System by Vicon Peak, Centennial, Colorado. Fastrack System by Polhemus 3Space, Colchester, Vermont. ANKLE DORSIFLEXION/PLANTARFLEXION COMPONENTS OF PRONATION/SUPINATION The dorsiflexion and plantarflexion components of ankle pronation and supination may be measured using a variety of techniques and landmarks. The most common proximal landmark used for these measurements is the fibular shaft,14 with the axis of the goniometer generally placed over, or distal to but aligned with, the lateral malleolus. Several distal landmarks have been used to measure ankle dorsiflexion and plantarflexion, including the shaft of the fifth metatarsal,4,34,4 and the plantar surface of the foot.4,11 Although each of these distal landmarks appears to be reliable in the measurement of ankle dorsiflexion, techniques employing the heel as a distal landmark are less reliable than those in which the fifth metatarsal or the plantar surface of the foot is used.4 Values obtained during the measurement of ankle dorsiflexion ROM have been shown to vary significantly according to the landmarks used during the measurement and according to the type of motion (active or passive) measured,4 reinforcing the need for standardized positioning and technique during the measurement of range of motion. The position of the patient’s knee during measurement also may influence the values obtained during dorsiflexion measurement, as tension in the calcaneal tendon may limit dorsiflexion with the knee extended.16 Many examiners recommend measuring the components of ankle motion, and in particular dorsiflexion, while maintaining the subtalar joint in a neutral position.3,4,9,47,48 The rationale behind such positioning is an attempt to minimize motion of the transverse tarsal joint while isolating talocrural motion.48 Although the use of neutral positioning of the subtalar joint during ankle dorsiflexion does not completely eliminate forefoot motion,3 a significant difference has been demonstrated in the amount of ankle dorsiflexion obtained when measurement is performed with the subtalar joint in the neutral compared with the pronated position.48 However, measurements of ankle dorsiflexion taken while the subtalar joint is maintained in neutral may require extensive examiner training to be reliable9 because of problems in the reliability of determining the neutral position of the subtalar joint.12,37 The literature describes a variety of methods of measuring range of motion of inversion and eversion that occur as the principal components of supination and pronation at the subtalar joint. If one attempts to isolate and measure the amount of inversion and eversion that occur only at the subtalar joint, one must make the decision whether or not to reference the motion from the neutral position of the subtalar joint (STJN). This position of the subtalar joint, STJN, is the position of the joint in which it is neither pronated nor supinated.42 Many individuals advocate measuring subtalar joint motion from a reference point of STJN23,45; others use anatomical zero as a reference.13,30 Unless the examiner is highly trained in determining the neutral position of the subtalar joint, measurements of subtalar motion referenced from subtalar neutral may be less reliable than those referenced from anatomical zero.9,12 Should one choose to reference measurements of subtalar motion from STJN, two basic methods may be used to establish the neutral position of the subtalar joint. One method uses a mathematical calculation based on measurements of calcaneal inversion and eversion to determine subtalar neutral,52 whereas the other method establishes subtalar neutral by palpating for talonavicular congruency.30 Because there is no general agreement as to which of these two techniques for establishing STJN is preferred, and because the latter technique requires fewer steps and has been reported to have good inter-rater reliability,49 palpating for talonavicular congruency is used in this text to determine STJN. To establish STJN by palpation, grasp the medial and lateral sides of the talar head with the thumb and index finger of one hand while passively pronating and supinating the foot with the other hand until the talar head is felt equally against the thumb and the index finger. This position of the talus is STJN. Once the neutral position of the subtalar joint has been located, measurement of inversion and eversion is performed by placing the axis of the goniometer on the posterior aspect of the subtalar joint at the level of the malleoli, aligning the proximal arm with a line bisecting the lower leg, and aligning the distal arm with a line bisecting the calcaneus. These measurements may be taken with the subject standing in a weight-bearing position or prone in a non–weight-bearing position, with the amount of motion obtained varying significantly depending on the patient’s position.23 Clinically, extension of the first MTP joint is the motion of the toes of most common concern, as limitation of that motion can cause significant impairment of foot function during gait. In fact, only articles examining MTP extension,6,15 and none examining MTP flexion or IP flexion or extension, were found in the literature. The focus in the literature on measuring MTP extension is probably due to the need for sufficient MTP extension, more than for other motions of the toes, in normal functioning of the foot. No fewer than four different methods of measuring extension of the first MTP joint have been described in the literature.6,15 These methods vary according to the technique used by the examiner and according to the position in which the patient is placed during the measurement. Two basic measuring techniques and a variety of patient positions are described in the four methods. The measuring technique described in this text uses an approach in which motion is measured from the medial aspect of the joint, with the goniometer aligned so that the axis is at the medial joint line, the moving arm is positioned along the medial midline of the proximal phalanx of the great toe, and the stationary arm is positioned along the medial midline of the first metatarsal. However, dorsal alignment of the goniometer also can be used. Subjects may be placed in a variety of positions when these measuring techniques are used, including non–weight-bearing and partial weight-bearing with the subject seated, and weight-bearing with the subject standing.15 Ankle Supination: Plantarflexion Component Supine or sitting (see Note), with knee flexed (as shown) or extended, and ankle in anatomical position (Fig. 13-7). After instructing patient in motion desired, plantarflex patient’s ankle through available ROM. Return to starting position. Performing passive movement provides an estimate of the ROM and demonstrates to patient exact motion desired (see Fig. 13-8). Palpate following bony landmarks (shown in Fig. 13-7), and align goniometer accordingly (Fig. 13-9). Perform passive, or have patient perform active, ankle plantarflexion (Fig. 13-10).
MEASUREMENT of RANGE of MOTION of the ANKLE and FOOT
ANKLE, SUBTALAR, AND TRANSVERSE TARSAL JOINTS
OSTEOKINEMATICS
ARTHROKINEMATICS
LIMITATIONS OF MOTION
METATARSOPHALANGEAL AND INTERPHALANGEAL JOINTS
OSTEOKINEMATICS
ARTHROKINEMATICS
LIMITATIONS OF MOTION
CAPSULAR PATTERN
ROM AND FUNCTIONAL ACTIVITY
TECHNIQUES OF MEASUREMENT
SUBTALAR INVERSION/EVERSION OF COMPONENTS OF PRONATION/SUPINATION
METATARSOPHALANGEAL AND INTERPHALANGEAL FLEXION/EXTENSION
Related posts:
 RELIABILITY and VALIDITY of MEASUREMENTS of RANGE of MOTION and MUSCLE LENGTH TESTING of the UPPER EXTREMITY
MEASUREMENT of RANGE of MOTION and MUSCLE LENGTH: CLINICAL RELEVANCE
MEASUREMENT of RANGE of MOTION of the KNEE
RELIABILITY and VALIDITY of MEASUREMENT of RANGE of MOTION for the SPINE and TEMPOROMANDIBULAR JOINT
MEASUREMENT of RANGE of MOTION of the HIP
PEDIATRIC RANGE of MOTION
RELIABILITY and VALIDITY of MEASUREMENTS of RANGE of MOTION and MUSCLE LENGTH TESTING of the UPPER EXTREMITY
MEASUREMENT of RANGE of MOTION and MUSCLE LENGTH: CLINICAL RELEVANCE
MEASUREMENT of RANGE of MOTION of the KNEE
RELIABILITY and VALIDITY of MEASUREMENT of RANGE of MOTION for the SPINE and TEMPOROMANDIBULAR JOINT
MEASUREMENT of RANGE of MOTION of the HIP
PEDIATRIC RANGE of MOTION
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree