CHAPTER 27 Os Acromiale
PREOPERATIVE CONSIDERATIONS
Os acromiale is an uncommon anatomic anomaly that can be implicated in symptoms of rotator cuff pathology. It was recognized as an anatomic anomaly over 140 years ago,1 but its relevance in shoulder pathology and its treatment remain a point of controversy. The reported incidence of os acromiale varies from 1.5% to 15% in the population,2–4 but the incidence of os acromiale has not been noted to be higher in patients with impingement or rotator cuff disease. Does the presence of an os acromiale create a disadvantageous biomechanical situation that leads to impingement and rotator cuff tears? Regardless of the incidence of os acromiale in rotator cuff pathology, the surgeon is bound to encounter this association and will be faced with a surgical decision. An open fusion of the os acromiale with internal fixation can restore normal acromial anatomy and avoid the deltoid dysfunction produced by the open excision of large fragments,5–7 but the advent of arthroscopic management of impingement and rotator cuff tears has produced a new paradigm for the surgeon. Open reduction and internal fixation may be able to preserve these large fragments, but not without significant morbidity, the risk of nonunion, and the frequent need for hardware removal. It is difficult to resort to the open treatment of impingement and rotator cuff tears when arthroscopic subacromial decompression and arthroscopic rotator cuff repair are now the new standard of care in the treatment of rotator cuff disease. When an os acromiale is diagnosed in conjunction with rotator cuff disease, the arthroscopic resection or near-complete resection of the os has been shown to be effective, without any deleterious effect on the deltoid.8,9
ANATOMY AND PATHOANATOMY
Os acromiale is the result of failure of fusion of the acromiale apophyses. The resulting failure can produce two distinct physiologic types of os acromiales, a synchondrosis with a nonmobile os or pseudoarthrosis with a mobile os. The former is stable and does not require operative treatment; the latter is unstable, with a resulting step-off, and is cause for concern in the presence of impingement and/or rotator cuff tears.7 The pseudoarthrosis can be hypertrophic, presenting an irregular inferior surface to the rotator cuff.
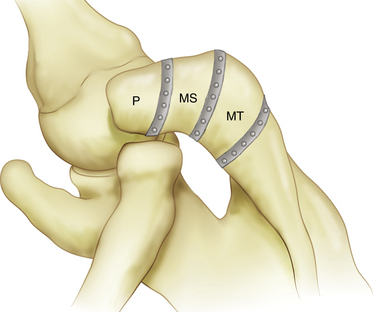
Three ossification centers of the acromion appear between the ages of 15 and 18 years and fuse with the scapula between the ages of 22 and 25 years.9 There are three potential areas of nonunion and thus three types of os acromiales (Fig. 27-1), but there is lack of agreement on the location of these areas of nonunion. The preacromion is the smallest of the os and its posterior margin is located at or anterior to the midpoint of the distal clavicle. The mesoacromion is defined by its posterior margin, which is in line with the posterior margin of the clavicle and acromioclavicular joint. The meta-acromion is the largest of the os and its posterior margin is located close to the lateral aspect of the scapular spine.8,10 The mesoacromion is the most common and is the primary subject of discussion. The preacromion is the next most frequently encountered and its excision is without consequence. The meta-acromion is uncommon, but the incidence and occurrence of these different types are uncertain. There is considerable variability in the location of the pseudoarthrosis site, which can occur anywhere within the developing acromion, so how each author defines the types of os acromiales treated also varies.4–9
DIAGNOSTIC IMAGING
Os acromiale is readily visualized on standard radiographs, as well as on computed tomography (CT) and magnetic resonance imaging (MRI) scans. An anteroposterior (AP) x-ray view demonstrates a double contour because the os is superimposed over the remaining posterior acromial bone (Fig. 27-2). Outlet and axillary x-ray views can also show the os. MRI better defines the os and can also demonstrate the status of the underlying cuff. Os acromiale is best seen on MRI axial views (Fig. 27-3).






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


