CHAPTER 3 Shoulder Biomechanics, Examination, and Rehabilitation Principles
Orthopedic surgeons frequently rely only on the evaluation of the musculoskeletal system to arrive at a clinical diagnosis. Although this is reliable in assessing acute injuries, deficits in the sensorimotor system, which consists of posture, postural stability, muscle tone, and movement patterns, play a significant role in the development of chronic musculoskeletal pain and therefore must be included in the consideration of cause.1
SHOULDER BIOMECHANICS
The Shoulder in the Kinetic Chain
The shoulder complex functions as part of a kinetic chain, which is defined as a series of links and segments activated sequentially in a coordinated fashion to generate and transmit forces to accomplish a specific function.2,3 An example of a kinetic chain is the childhood game crack the whip, wherein a group of children hold hands in a line to try to accelerate the last child by creating a whip effect. Each child represents a segment of the chain and their joined hands represent links that sequentially create increased energy, force, and velocity. In activities that use a throwing motion (e.g., pitching or tennis), there is proximal to distal muscle activation and coordination of body segments producing interactive moments at the terminal segment (hand or racket).4,5 The initiating ground reaction force is increased as it is transmitted through the knees and hips through the large muscles of the legs into the lumbopelvic region and the rest of the trunk. The proximal segments—that is, the legs and trunk—produce roughly half the energy (51%) and force (54%) that is ultimately delivered to the distal end of the kinetic chain.6,7 The scapula and glenohumeral joint function as both a link and segment in the chain, increasing the kinetic energy and force generated, and as a conduit to funnel and transmit these forces to the distal segments.
When an individual reaches, pushes, or pulls from a sitting position, there is less energy and force contribution from the legs, and the primary generator for upper extremity motion is the initiation of trunk stabilization. Coordinated muscle activation sequences result in movement patterns, which create joint motions to efficiently accomplish specific tasks. These diagonal activation patterns create a “serape effect” from the knee or lumbopelvic region to the shoulder,8 act locally on one joint or harmonize several joints, provide cocontraction force couples that control joint perturbations and provide stability, and generate and transmit force. This allows the scapular stabilizing muscles to position the scapula optimally for shoulder function and for the rotator cuff to compress and position the humeral head in the glenoid fossa.
The Scapula in Shoulder Function
The scapula provides anatomic and kinematic connections between the torso and upper extremities. The shoulder muscles can be classified anatomically by their origins and insertions into the axioscapular, scapulohumeral, and axiohumeral group. The axioscapular muscles that attach the scapula to the thorax include the serratus anterior, trapezius, rhomboids, levator scapulae, and pectoralis minor. These scapular stabilizing muscles position the scapula optimally for the humeral head. The serratus anterior and trapezius muscles are so large that the muscle fibers course in different directions and, as a result, both muscles have multiple functions that relate to activity and arm position.9 The scapulohumeral group consists of the supraspinatus, infraspinatus, teres minor, subscapularis, deltoid, and teres major. The rotator cuff muscles provide concavity or compression at the glenohumeral joint and fine-tune humeral head rotation and depression in an attempt to keep the humeral head centered in the glenoid throughout the arc of upper extremity motion. The axiohumeral muscles, the pectoralis major and latissimus dorsi, are the considered the power muscles of the shoulder. Shortening or tightness of these muscles is frequently associated with abnormal glenohumeral kinematics. The biceps and triceps comprise a special category, because they extend from the scapula to the forearm.
The shoulder complex is an important kinematic link between the trunk and arm, providing a stable platform for arm rotation during throwing. The scapulothoracic articulation, and the glenohumeral, acromioclavicular, and sternoclavicular joints, form two individual but paired mechanisms, one an open chain and one a closed chain.10 A closed kinetic chain, such as the one formed by the thorax, scapula, and clavicle, is defined by the terminal link being fixed or immovable. The glenohumeral joint is an open kinetic chain mechanism, allowing movement of the hand as the terminal link. Normal shoulder function and scapulohumeral rhythm require that all four articulations participate in a simultaneous, synchronous, and coordinated manner, and that the muscles controlling them are activated in the correct succession.
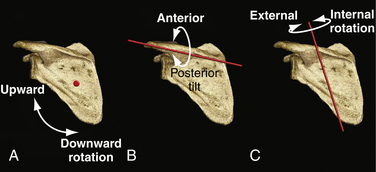
Scapular motions include upward and downward rotation in the coronal plane about an anterior-posterior axis (Fig. 3-1A), anterior and posterior tilting in the sagittal plane about a medial-lateral axis (see Fig. 3-1B), and internal and external rotation in the transverse plane about a vertical axis (see Fig. 3-1C). In addition, there are translations of the clavicle and thus of the scapula, in the superior and inferior directions (scapular movement along the vertical axis), as well as in protraction and retraction or abduction and adduction (scapular movement along the medial-lateral axis). Several investigators have shown that during glenohumeral elevation, the normal scapula demonstrates upward rotation, external rotation, and posterior tilting and translates into a more superior and posterior position.11,12
The scapular stabilizing muscles function as force couples to control the motions of the scapula. A force couple is formed when two forces act in opposite directions to impose rotation about an axis. The serratus anterior controls the movements of internal rotation, upward rotation, anterior tilting, and lateral translation when it fires concentrically, and external rotation, downward rotation, and posterior tilting when it fires eccentrically, depending on shoulder position.13 The upper and lower trapezius and rhomboids counteract this. Scapular elevation is a function of the upper trapezius, levator scapula, and the upper fibers of the serratus anterior. This is counterbalanced by the scapular depression resulting from the functions of the lower portions of the trapezius and serratus anterior.9,14
The Scapula in Shoulder Dysfunction
Abnormal scapular kinematics occur as a result of alterations in anatomy, physiology, and/or biomechanics, or musculoskeletal adaptations to these aberrations, and can usually be classified as being proximally or distally derived (Box 3-1).15 The appropriate term to describe the abnormal scapular movements that occur when the shoulder is moved voluntarily is dyskinesis, as opposed to abnormal involuntary movements, such as in cerebral palsy or Parkinson’s disease, which represent what is termed dyskinesia. When the basic problem occurs proximally and posteriorly to the glenohumeral joint, the observed scapular dyskinesis is considered proximally derived (PDSD). When an abnormality of the glenohumeral joint, subacromial space, clavicle, or acromioclavicular or sternoclavicular joints occurs, the resulting dyskinesis that is usually observed is considered distally derived (DDSD). The exception to this classification is the presence of shortening or tightness of the pectoralis minor or clavipectoral fascia, which fits best into PDSD, despite its anterior position. In the context of the kinetic chain, proximally derived scapular dyskinesis is associated with proximal link or segment weakness or interruption, whereas distally derived dyskinesis is the result of recoil or kickback from a distal link or segment dysfunction. This has important implications for the treatment of shoulder and upper extremity conditions.
Box 3-1 Causes of Scapular Dyskinesis
PDSD is frequently associated with postural dysfunction. The classic presentation is that of the patient who sits or stands with the head in a forward position, with focal cervical lordosis (usually at C5-C6), thoracic kyphosis, anterior tilt, and internal rotation of the scapula and humeral head.1 The anterior tilt is typically associated with tightness or shortening of the pectoralis minor muscle tendon unit, whereas the internal rotation of the humeral head usually results from tightness or shortening of the latissimus dorsi, teres major, pectoralis major, and/or subscapularis.16,17
Proximal kinetic chain weakness can be caused by abnormalities of the lower extremities, lumbopelvic, lumbar, or thoracolumbar deficits. Lumbopelvic weakness with resulting core instability appears to be one of the most common causes of proximally derived scapular dyskinesis in the throwing athlete.8 Lumbar lordosis with poor control of the abdominal musculature is frequently associated. Injury to the long thoracic nerve or, less commonly, the spinal accessory nerve, causes weakness and atrophy of the serratus anterior and trapezius, respectively. Long thoracic stretch mononeuropathy is actually more common in overhead athletes than previously thought, and recently has been associated with the use of heavy backpacks by children and young adults (backpack palsy). When these muscles are compromised from neurologic interruption or fatigue, force couple imbalances ensue, and a significant adverse cascade of events occurs (Fig. 3-2). Proprioception is altered, a dyssynchronous muscle firing pattern occurs, and there is an abnormal increase in scapular mobility, which is usually manifested as a loss of external rotation control, with subsequent increased stress on the glenohumeral joint capsule, glenoid labrum, and rotator cuff.18–20 Increased protraction (scapular internal rotation and anterior tilt) has been shown specifically to increase the strain on the anterior band of the inferior glenohumeral ligament and decrease anterior translation of the humeral head.20 Optimum rotator cuff activation occurs only in the presence of a scapula that is optimally positioned for stability. As a result of scapular dyskinesis, there are increased intrinsic joint loads and decreased force delivered to the terminal segment.4
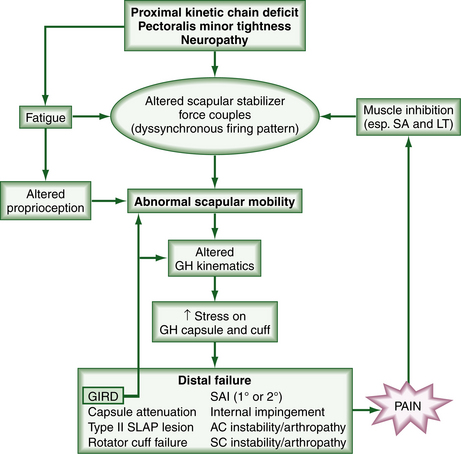
Distally derived scapular dyskinesis is very common and is associated with an array of pathologic conditions.7,18,21-24 Related intra-articular pathology may include labral tears or detachments, capsular attenuation or tears (with resultant instability), focal capsular restrictions such as glenohumeral internal rotation deficit (GIRD) commonly seen in overhead athletes, biceps lesions, adhesive capsulitis, and glenohumeral arthritis. Rotator cuff tendinitis and tears, primary impingement syndrome, and calcific tendinitis have been observed to be associated with scapular malposition. In these cases, the pain and altered biomechanics associated with the pathology appear to cause selective inhibition of the serratus anterior and lower trapezius, with the subsequent events outlined earlier. When glenohumeral internal rotation deficit (GIRD) is present, there is a direct consequence of altered scapular mobility. In any case, there results a vicious cycle of scapular dysfunction and shoulder pathology (see Fig. 3-2).
Subacromial impingement syndrome has historically been associated with abnormal acromial morphology25; however, recent observations have attributed the decrease in the subacromial space height to be more frequently related to a variety of factors that affect scapular position. For example, with increased thoracic kyphosis, there is elevation and anterior tilting of the scapula at rest, decreased upward rotation and posterior tilt of the scapula with glenohumeral elevation, decreased elevation of the glenohumeral joint, and decreased force generated at 90 degrees of scapular plane abduction.26 In addition, it has been shown that with cervical spine flexion of 25 degrees, there is an increase in scapular upward rotation and a decrease in posterior tilting in healthy subjects. Meskers and colleagues27 have demonstrated that the supraspinatus outlet narrows during elevation in the frontal plane from 30 to 130 degrees; however, with external rotation and movement in the horizontal plane, the greater tuberosity moves away from the coracoacromial ligament. Borstad and Ludewig have shown an association between subacromial impingement and anterior tilting, increased internal rotation, and decreased upward rotation of the scapula.28 Cools29,30 has shown that patients with subacromial impingement demonstrate a decrease in peak force for isokinetic protraction, decreased protraction-to-retraction ratio, and decreased electromyographic activity in the lower trapezius, as well as abnormal muscle recruitment in overhead athletes, with delayed activation of the middle and lower trapezius.




