CHAPTER 29 Scapulothoracic Burscoscopy
The scapulothoracic articulation plays a crucial role in the motion of the upper extremity. There are multiple disorders that affect this articulation and cause snapping scapula. Snapping scapula may be secondary to scapulothoracic bursitis, scapular osteochondromas or elastofibromas, scapular winging, scapulothoracic dyskinesia, and/or Sprengel’s deformity. The term snapping scapula is somewhat of a misnomer because not all disorders of the scapulothoracic joint make a characteristic snapping sound. As the understanding of snapping scapula improves, more cases are being diagnosed and treated. In most cases, conservative management is successful.1 However, patients who fail conservative management may be treated with open or arthroscopic surgery. Historically, surgical procedures described were open procedures2–8 or a combined open and arthroscopic procedure.4 An all-arthroscopic procedure was initially described by Cuillo in 1992 and the first series was later published by Harper and colleagues.2,10 Scapulothoracic burscoscopy provides a safe alternative to open superomedial angle resection, bursectomy, and excision of an elastofibroma or osteochondroma.
ANATOMY AND PATHOANATOMY
Anatomy
The scapula is a triangular-shaped bone that articulates with the humerus and clavicle laterally and thorax ventrally. Its only attachment to the axial skeleton is the acromioclavicular joint. The scapula is integral to motion of the shoulder because it provides a congruous joint for humeral articulation, glides on the thorax to position the glenoid in space,12 and serves as a stable base for the origin and insertion of multiple muscles that control scapular and humeral motion.
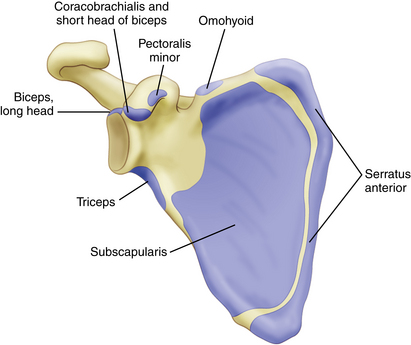
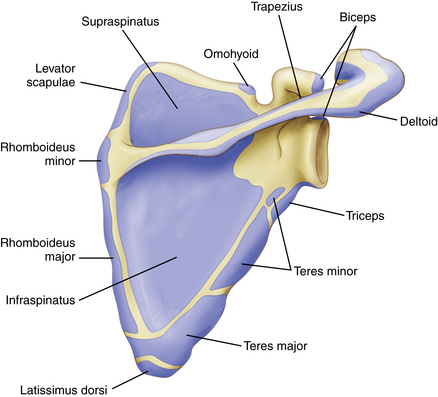
Seventeen muscles have their origins or insertions on the scapula (Box 29-1). The subscapularis muscle covers the anterior surface of the scapula and the supraspinatus and infraspinatus cover the posterior surface in the supraspinatus and infraspinatus fossa, respectively. The scapular spine and acromion provide the origin of the deltoid muscle and an insertion for the trapezius muscle. On the medial border, the serratus anterior, levator scapulae, and rhomboid major and minor muscles attach to the scapula. The lateral border is the origin of the triceps, teres major, and teres minor muscles. Inferiorly, the latissimus dorsi muscles attaches to the inferior angle of the scapula. Other muscle attachments include the omohyoid, long head of the biceps, coracobrachialis, short head of the biceps, and pectoralis minor muscles (Figs. 29-1 and 29-2).
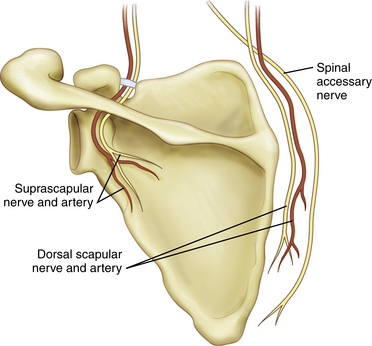
The neurovascular structures that are in proximity to the scapula include the suprascapular nerve and artery, dorsal scapular nerve and artery, transverse cervical artery, spinal accessory nerve, and long thoracic nerve. The suprascapular nerve travels through the suprascapular notch and suprascapular artery over the transverse scapular artery to continue laterally around the spine of the scapula and through the spinoglenoid notch into the infraspinatus fossa. The dorsal scapular nerve dorsal scapular artery,13 and spinal accessory nerve (cranial nerve IX) travel parallel to the medial border of the scapula. Understanding these relationships will allow safe portal placement and minimize the risk of injury to important neurovascular structures when performing scapulothoracic burscoscopy (Fig. 29-3).
There are two major anatomic bursa and four minor adventitial bursae of clinical significance. The anatomic bursae are the supraserratus bursa, which is located between the subscapularis and serratus anterior muscles, and the infraserratus bursa, which is located between the serratus anterior muscle and chest wall.1,3,6,11,14 These bursae have been consistently located in both cadaveric specimens and during arthroscopic procedures (Table 29-1; Figs. 29-4 and 29-5).
TABLE 29-1 Bursae of the Scapulothoracic Joint
| Bursae | Location |
|---|---|
| Supraserratus bursa | Between serratus anterior and subscapularis muscles |
| Infraserratus bursa | Between chest wall and serratus anterior muscle |
| Supraserratus bursa (superomedial angle) | Between serratus anterior and subscapularis muscles |
| Infraserratus bursa (superomedial angle) | Between chest wall and serratus anterior muscle |
| Infraserratus bursa (inferior angle of scapula) | Between chest wall and serratus anterior muscle |
| Trapezoid bursa | Between spine of the scapula and trapezius muscle |
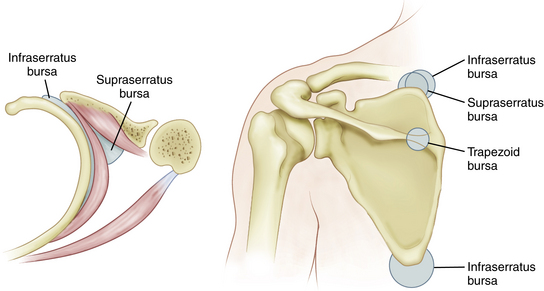
FIGURE 29-4 Major (anatomic) and minor (adventitial) bursae of the scapulothoracic joint and its orientation in relation to the chest wall, scapula, serratus anterior muscle, and subscapularis muscle.
(Adapted from Kuhn JE, Hawkins J. Evaluation and treatment of scapular disorders. In: Warne JJP, Iannotti JP, Gerber C, eds. Complex and Revision Problems in Shoulder Surgery. Philadelphia: Lippincott-Raven; 1997:357-375.)
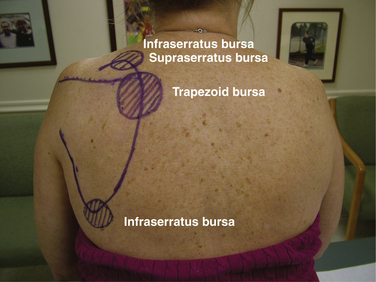
In addition, four adventitial bursae have been described. These are thought to develop as a result of scapulothoracic dyskinesia and are not consistently seen. The supraserratus and infraserratus bursae (minor) are located ventral to the superomedial angle of the scapula. A second infraserratus bursa is located anterior to the inferior angle of the scapula. The trapezoid bursa is located dorsal to the spine of the scapula.14
Pathoanatomy
The differential diagnosis of snapping scapula can be divided into bony or soft tissues disorders. However, this categorization is purely arbitrary because bony causes may play a role in soft tissue disorders. Changes in bony anatomy of the scapula and thus incongruity of the scapulothoracic joint may cause a snapping scapula. Osteochondromas, Luschka’s tubercle, hooking of the superomedial scapula, elastofibroma, malunion of scapular or rib fractures, and callous formation after scapular or rib fractures have been reported to be a cause of the snapping scapula.1,5,6,8,15-18 The resultant change in anatomy may create sounds that vary from a barely audible friction rub to a loud snapping sound.5,20–22 There is no consensus on whether anatomic changes or the resulting bursitis are the source of the periscapular pain.
In addition to soft tissue and bursal inflammation,21 scar formation after periscapular muscle avulsions may cause incongruity between the scapula and chest wall and cause periscapular crepitus or an audible snapping sound. However, symptomatic bursitis does not necessarily have an accompanying audible sound. On the contrary, a snapping scapula is not necessarily symptomatic and thus may not be clinically significant.
HISTORY AND PHYSICAL EXAMINATION
The patient with a symptomatic snapping scapula often gives a history of a traumatic event or a repetitive upper extremity activity.4,10,23–28 The traumatic event may involve a protraction or retraction movement of the scapula, direct blow to the scapula, fracture of the scapula, or fracture of the underlying rib cage. Sports requiring repetitive or forceful shoulder activities including baseball pitching, swimming, weight training, gymnastics, football, and fencing may produce the symptoms of snapping scapula.
Regardless of the underlying pathology, most patients report having crepitus—grinding, grating, clicking, or crunching with shoulder motion.5,6,17,30 The audible snap may or may not be painful.31 We have noted that the crepitus associated with bursitis is less severe than crepitus or snapping caused by bony lesions.20 Pain is often localized to the superomedial angle or medial border of the scapula, but pain at the inferior angle of the scapula is more typical in overhead athletes.28 Patients commonly report pain that is worsened with overhead activities, irrespective of the location of the inflamed bursa. Some patients may report a family history of similar symptoms.23
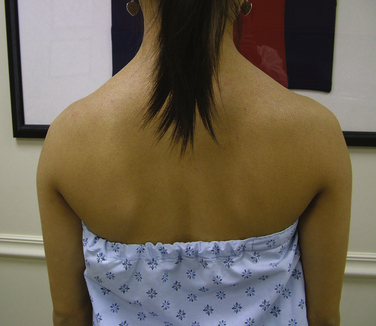
Physical examination findings associated with disorders of the scapulothoracic articulation can vary from near-normal to severe scapular winging and crepitus. Inspection of the posterior aspect of the shoulders may reveal subtle asymmetry. The dominant shoulder is frequently slightly depressed compared with the contralateral shoulder.32 This is a normal finding in many active individuals and athletes and is not directly related to a snapping scapula (Fig. 29-6).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


