CHAPTER 10 Arthroscopic Acromioclavicular Joint Reconstruction
PREOPERATIVE CONSIDERATIONS
Anatomy of the Native Acromioclavicular Joint
The AC joint complex is a stout articulation anchoring the clavicle and scapula. It provides a pivot point where the clavicle and axial skeleton articulate with the complex motions of the scapula. The complex includes the AC joint proper and the coracoclavicular ligaments. The AC joint proper is a diarthrodial joint that rotates and translates in superior-inferior and anterior-posterior directions. Each side of the joint is covered by hyaline cartilage, with a meniscus-like disk of fibrocartilage interposed. The meniscus-like disk has tremendous variation in size and shape. The exact function of the intra-articular disk is unknown; it has been shown to degenerate with age and to be almost functionless beyond age 40.1–3 The capsule and stabilizing ligaments surround the joint, providing stability.
Multiple structures enhance the stability of the AC joint. Primary static stabilizers are the AC joint ligaments (anterior, posterior, superior, and inferior) and the coracoclavicular ligaments (conoid and trapezoid). Dynamic stabilizers include the deltoid and trapezius muscles. The superior AC ligament has confluence fibers with the enveloping deltotrapezial fascia, which add stability of the joint in motion.4
Horizontal translation of the distal clavicle is restricted mainly by the joint capsule and surrounding AC joint ligaments. Fukuda and colleagues5 have demonstrated that the superior and posterior ligaments contribute approximately 50% and 25% of the resistance, respectively, to posterior translation. This is an important consideration when performing an arthroscopic distal clavicle resection. To avoid the potential complication of posterior impingement of the distal end of the resected clavicle on the spine of the scapula, every effort should be made to preserve the superior and posterior capsule.
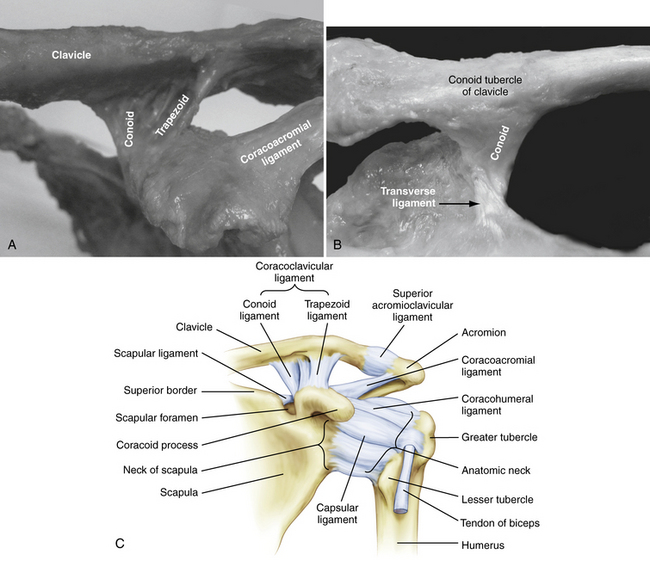
The coracoclavicular (CC) ligament complex is comprised of two ligaments.6 As the name implies, the general shape of each is cone-shaped and trapezoidal. Both ligaments are ribbon-like in dimension. The conoid ligament originates on the coracoid posterior to the pectoralis minor and inserts on the clavicle at an average of 46 mm from the distal end. This measurement is to the midportion, or mean, of the ligament insertion. The origin lies on the most posterior and medial portion of a previously unnamed tubercle of the coracoid, sometimes referred to as the knuckle. The insertion is linear and broad, fanning out along the most posterior border of the clavicle in the coronal plane. The clavicle has a small posterior protuberance called the conoid tubercle, where most of the conoid fibers attach. The trapezoid ligament originates just anterior and lateral to the conoid, again on the coracoid knuckle or tubercle. In contrast to the conoid, the trapezoid angles 45 degrees laterally to insert at an average distance of 26 mm from the distal end of the clavicle.4 Its ribbon-like form is oriented in the sagittal plane and is essentially orthogonal to the conoid. Its insertion on the clavicle is linear, spanning the entire width in the anterior to posterior direction. The conoid has been reported to have a more posteromedial origin from the coracoid whereas the trapezoid’s origin on the coracoid lies more anterior and lateral.7 The ligaments span a distance of approximately 1.1 to 1.3 cm and prevent inferior translation of the scapula relative to the clavicle.8 In the absence of AC joint ligaments, the CC ligament complex becomes an important secondary stabilizer of horizontal translation, especially to posterior displacement9 (Fig. 10-1).
Motion of the AC joint is complex and not completely understood. What has been made clear is that the scapula and clavicle have obligatory coupled motion around three axes that is guided by the AC joint and CC ligament complex. Rigid fixation of the AC joint with coracoclavicular screws prevents normal scapulathoracic motion and function.10
Biomechanics of the Acromioclavicular Joint
The biomechanics of native and numerous stabilization and/or reconstruction techniques has been extensively studied and is beyond the scope of this chapter. The native CC complex has been shown to have a biomechanical ultimate load of 500 to 725 N.11–13 The Weaver-Dunn procedure, with its various modifications, has gained much exposure. Despite its popularity, the transferred coracoacromial (CA) ligament has an ultimate load of only 145 N,13 which appears insufficient in strength and stiffness when compared with the native ligament complex.12,14 This may account for the high number of failures reported with its use.15,16
Mazzocca and associates, 17 after reviewing recent biomechanical data, reached several conclusions. First, the popular CA ligament transfer provides only 25% of the strength of the intact CC ligament complex but the biomechanical strength can be improved with synthetic augmentation. The CA ligament transfer, even with suture augmentation, has no effect on anterior-posterior displacement. Finally, the use of a free tendon graft can provide improved initial stability and equivalent strength to the native ligament complex; this represents a biomechanical improvement compared with the traditional CA ligament transfer. It is findings such as these that have prompted the development of the techniques described in the following sections, including the GraftRope (Arthrex, Naples, Fla) and ACCR.
Mechanism and Classification of Acromioclavicular Joint Separations
AC joint injuries were first recognized and described by Hippocrates.18 Cadnenat, in 1917, described the sequential failure of AC ligaments, coracoclavicular ligaments and, finally, the deltoid and trapezial fascia.19 Tossy and associates20 have proposed a classification system describing three grades of injury to the AC joint. Rockwood and coworkers21 later expanded the classification to include six grades, and this has become the universally accepted classification system.
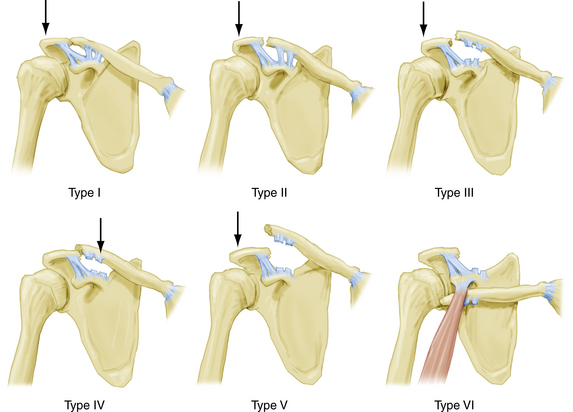
Type I injuries are essentially AC joint sprains to the AC ligaments and capsular complex. There is no instability of the AC joint. Type II injuries represent rupture of the AC ligaments and joint capsule with intact CC ligaments. Significantly more force is required for this injury pattern. Generally, less than 50% superior displacement of the clavicle is common, although instability in the anterior-posterior direction is a more consistent finding. Type III injuries occur when both AC and CC ligament complexes are disrupted. There is complete loss of contact between the clavicle and acromion, with 100% displacement. With type IV injuries, there is complete disruption of the AC and CC ligaments, with posterior displacement into or through the trapezius. Type V injuries represent significantly displaced type III injuries, with 100% to 300% displacement, secondary to complete rupture of the deltotrapezial fascia. Finally, the rare type VI injury represents a complete dislocation, with the clavicle displaced inferior, locked beneath the acromion or coracoid process (Fig. 10-2).
History and Physical Examination
The most commonly observed symptom in acute AC joint disruptions is anterosuperior shoulder pain. The pain may be poorly localized at times because of the unique innervations of the AC joint. The AC joint is innervated by both the lateral pectoral nerve and branches off the suprascapular nerve. The pain is usually referred to the anterosuperior shoulder in the region of the AC joint and clavicle, anterior brachium, and anterolateral neck.
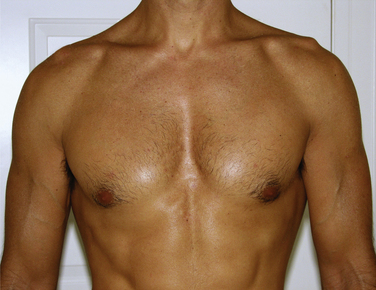
In general, the physical examination should begin with unobstructed observation of the patient in the seated position, with the arms held relaxed at the side. Inspection and comparison with the unaffected shoulder and direct palpation will reveal a variable amount of tenderness and deformity. Injury to the AC joint can be identified by localizing pain to the AC joint by direct palpation and/or provocative maneuvers. The diagnosis can be further confirmed by the relief of symptoms following AC joint injection of local anesthetic.10
Physical Findings by Rockwood’s Classification
Type I Injuries.
No deformity would be expected with type I injuries, and often the only positive examination finding is pain with palpation. The AC ligaments have sustained a traction injury but, along with the CC ligament complex, they remain intact. Patients may also complain of pain with the cross-arm adduction maneuver. This test is performed in the seated position with the elbow elevated and flexed to 90 degrees. The arm is brought across the chest compressing the AC joint and will cause discomfort, specifically over the AC joint when positive. O’Brien and colleagues22 have described a useful test to help distinguish pain originating from the AC joint and pain caused by superior labral pathology. The test is performed by adducting the arm in 90 degrees of forward elevation and providing a downward force while resisted by the patient. Reproducible superior shoulder pain while the patient’s arm is in full external rotation implies AC joint pathology, whereas pain or painful clicking described as inside the shoulder with the arm in internal rotation is considered indicative of labral abnormality. Radiographs will be normal.
Type III Injuries.
These injuries represent a complete disruption of both AC and CC ligament complexes. The clavicle remains in its relatively normal position because the deltoid and trapezial fascia remains intact but the acromion, scapula, and upper extremity displace inferiorly. The clavicle is unstable in both the horizontal and vertical planes and deformity is obvious on inspection. Range of motion is painful and may elicit palpable crepitus. The palpable bump of the AC joint may reduce by asking the patients to shrug their shoulders. There is usually a 100% displacement of the clavicle relative to the acromion on radiographic evaluation (Fig. 10-3).
Type VI Injuries.
These injuries are rare injuries that are thought to result from severe trauma.23 The clavicle can become wedged beneath the acromion or coracoid. Deformity of the shoulder shows a prominent acromion, with loss of the normal rounded contour of the shoulder. Patients often have paresthesias of the affected arm. Although radiographs confirm the diagnosis, close attention to associated injuries may necessitate further imaging. Treatment is surgical reduction and stabilization. Most paresthesias will resolve with reduction of the clavicle.
Diagnostic Imaging
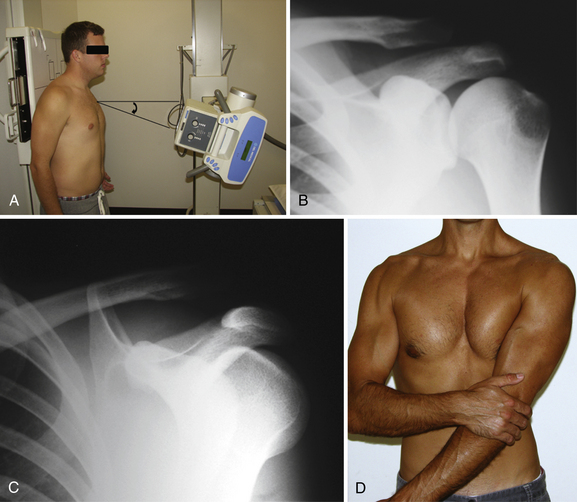
The Zanca view provides the most accurate assessment of the AC joint. This view is obtained by positioning the x-ray beam for a true AP of the shoulder, with an additional 10 degrees cephalad angulation.24 This eliminates the overlap of the scapular spine usually seen on standard AP films. Because the soft tissue overlying the AC joint is minimal compared with the glenohumeral joint, the x-ray penetration should be reduced by 30% to 50%. A properly performed Zanca view helps determine superior displacement, if any, of the clavicle. Taking bilateral simultaneous Zanca views provides easy and accurate comparison with the patient’s contralateral side. For subtle injuries, types I and II, bilateral measurements of the CC distance can be calculated (Fig. 10-4).
Bearden and associates8 have shown that the normal distance between the inferior aspect of the clavicle and superior aspect of the coracoid is 1.1 to 1.3 mm. This measurement will vary with changes in distance from the x-ray beam and cassette—hence the need for side to side comparisons. A difference of over 40% is considered diagnostic for a complete CC ligament disruption. It has also been reported that an elevation of just 25% to 50% compared with the unaffected side is indicative of a complete disruption.21

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


