CHAPTER 21 Large to Massive Rotator Cuff Tears
PREOPERATIVE CONSIDERATIONS
During the past 10 to 15 years, there has been a dramatic evolution in the arthroscopic treatment of massive rotator cuff tears. In the past, many massive rotator cuff tears (more than 5 cm in greatest dimension, as defined by DeOrio and Cofield1) were regarded as irreparable. Today, we have gone from being unable to repair any rotator cuff tears arthroscopically to being able to repair almost all rotator cuff tears, even massive ones, arthroscopically.
Massive rotator cuff tears make up approximately 20% of all cuff tears2 and a considerably greater percentage (80%) of recurrent rotator cuff tears.3 In the early 1990s, the recommendation often included simple débridement of the massive tears.4 Although débridement of massive tears has been relatively successful in terms of pain relief, overhead function is often not an attainable goal, particularly for patients who do not have balanced force couples.5,6
Advancement in arthroscopic shoulder surgery has now improved our understanding of tear patterns and has offered new opportunities and capabilities in terms of rotator cuff repair techniques.2 Understanding tear patterns is particularly important. Without a comprehensive understanding of tear patterns, the traditional repair techniques have focused on covering the hole. This was usually accomplished via an open or miniopen approach and subsequent extensive release of the cuff muscles to achieve enough mobilization to allow a repair to the bone. This medial to lateral technique did not respect the true pattern of pathology. Also, the extensive mobilization required can result in overtensioning of the rotator cuff and its subsequent failure.7 This can lead to damage to the suprascapular nerve, thereby leaving a repaired cuff completely nonfunctional.8 This may explain the traditionally poor results repairing primary and recurrent massive rotator cuff tears via an open approach1,9,10 or an arthroscopic approach based on a purely medial to lateral mobilization and repair.11
More recently, some have proposed the use of orthobiologic tissue patches to cover the hole in massive rotator cuff tears.12 Again, this approach does not respect the biomechanics of the rotator cuff and is therefore doomed to failure. Unless the rotator cuff tendons can be appropriately tensioned to achieve an optimal position along the muscle length-tension curve, ultimate improvement in function is unlikely.
Although truly irreparable rotator cuff tears do exist (tears with 75% or greater fatty infiltration),13 most patients with massive rotator cuff tears can obtain a good cuff closure and clinical result. The key to repairing the traditional irreparable tear is understanding the pattern of the tear and then knowing how to deal with each pattern. With a suitable knowledge of tear patterns and with adequate and appropriate mobilization and repair techniques (see later), most massive rotator cuff tears can and should be repaired. This leads not only to improved pain relief but also a return of a significant amount of function, usually including overhead function.2,3
PRINCIPLES AND ANATOMY
Force Couples
A primary function of the rotator cuff is to balance the force couples about the glenohumeral joint. A force couple is a pair of forces that act on an object and cause it to rotate. For any object to be in equilibrium, the forces must create moments about a center of rotation that are equal in magnitude and opposite in direction. In the situation in which the center of rotation is equidistant from the point of application of each force, the forces must be equal and opposite in direction for equilibrium to exist.
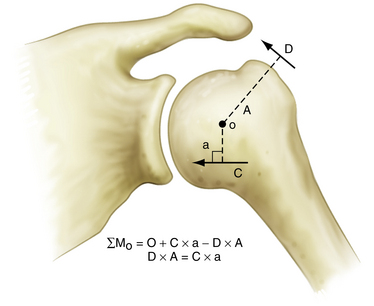
In the shoulder, the coronal plane force couple has been described by Inman and colleagues.14 This force couple is a result of the balance of moments created by the deltoid versus those created by the intact portions of the inferior rotator cuff (Fig. 21-1). During abduction, the coronal plane force couple will only be balanced if the line of action of the rotator cuff force is below the center of rotation of the humeral head, so that it can oppose the moment created by the deltoid. Balancing the coronal plane force couple is essential because this maintains a stable fulcrum for glenohumeral joint motion.
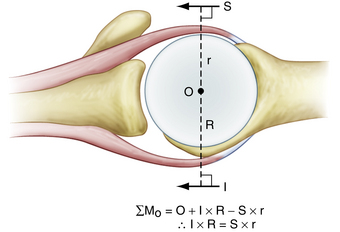
An equally important force couple is the transverse plane force couple. This force couple consists of the subscapularis anteriorly, balanced against the posterior rotator cuff (Fig. 21-2). This force couple is relevant in massive rotator cuff tears in which the tear may extend more posteriorly, leaving only a remnant of intact posterior cuff. In many cases, the posterior rotator cuff is so weak that it cannot balance the anterior moment created by the large subscapularis tendon. Furthermore, a large posterior rotator cuff tear can result in such a deficiency that the moment created by the inferior rotator cuff is also insufficient to maintain equilibrium in the coronal plane. This can then result in anterior and superior translation of the humeral head and the inability to maintain a stable fulcrum of motion. Therefore, when faced with a rotator cuff tear, the primary goal of surgery is to balance the force couples in the transverse and coronal planes and not necessarily to cover the hole. Again, the goal of rotator cuff repair is not to bring a medialized tendon stump laterally to bone, but to restore the balance of forces that control shoulder motion.
Rotator Cable-Crescent Complex: Suspension Bridge Analogy
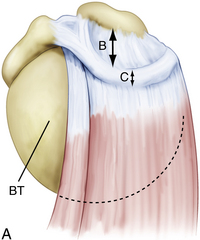
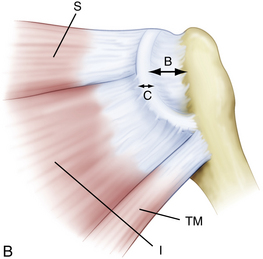
When arthroscopically viewed from the glenohumeral joint, the articular surface of the intact rotator cuff demonstrates an arching, cable-like thickening of the capsule surrounding a thinner crescent of tissue that inserts into the greater tuberosity of the humerus.15 This cable-like structure, which represents a thickening of the coracohumeral ligament, is consistently located at the avascular zone margin of the rotator cuff (Fig. 21-3). It extends from its anterior attachment into the greater tuberosity of the humerus, just posterior to the biceps tendon, to its posterior attachment near the inferior border of the infraspinatus. This rotator cable potentially serves a protective role by stress-shielding the thinner, avascular crescent tissue, analogous to a load-bearing suspension bridge.
Similar to the intact rotator cuff, a rotator cuff tear can also be modeled after a suspension bridge, in which the free margin of the tear corresponds to the cable and the anterior and posterior attachments of the tear correspond to the supports at each end of the cable’s span. This model would predict, and subsequent studies have shown, that despite a tear in the avascular zone of the supraspinatus tendon, the supraspinatus muscle could still exert a compressive effect on the glenohumeral joint by means of its distributed load along the span of the suspension bridge configuration. The study by Halder and associates16 supports the concept that in small and medium-sized rotator cuff tears, the rotator cuff muscle forces are effectively transmitted along the rotator cuff cable, bypassing the torn supraspinatus tendon. That is why certain rotator cuff tears, even massive ones, can demonstrate functional kinematics and why after rotator cuff repair, good results can be achieved, even when a water-tight closure is not obtained.11,17
Furthermore, the implication of the cable-crescent concept contradicts the historic principle of covering the hole, particularly when using techniques such as tendon transfers to obtain closure of massive, so-called irreparable, rotator cuff tears. Others have advocated the use of tendon transfers, including the infraspinatus and subscapularis, to cover rotator cuff defects in massive tears.17 Transferring these muscles superiorly, however, significantly alters the normal mechanics of the rotator cuff.
Tear Patterns
Crescent-shaped tears are the simplest of all tears and, although they can be massive, these tears do not typically retract medially to a significant degree. They demonstrate excellent mobility from a medial to lateral direction and can be repaired directly to bone, with minimal tension to the anatomic bone bed (Fig. 21-4).
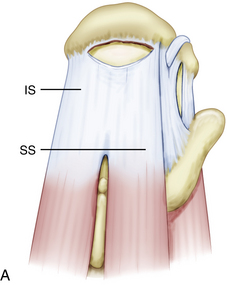
In contrast, U-shaped rotator cuff tears extend much farther medially than crescent-shaped tears, with the apex of the tear adjacent to or medial to the glenoid rim. Recognizing this tear pattern is critical, because attempting to mobilize and repair the apex of the tear to a lateral bone bed will result in overtensioning of the rotator cuff margin and subsequent failure. These tears demonstrate significant mobility from an anterior to posterior direction and should be initially repaired in a side to side fashion using the biomechanical principle of margin convergence (Fig. 21-5).
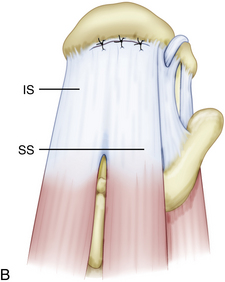
L-shaped and reverse L-shaped tears are similar to U-shaped tears. These are usually massive tears, with a longitudinal component in the direction of the fibers of the rotator cuff and a transverse component along the lateral cuff insertion (Fig. 21-6). One of the leaves is more mobile than the other leaf and can be easily brought to the bone bed.
These first three tear patterns represent about 90% of posterosuperior rotator cuff tears and can be repaired using the principles outlined here. Thus, most rotator cuff tears, even massive tears, can be repaired without extensive mobilization with an understanding and recognition of these tear patterns. Repairing tears according to their tear pattern can lead to excellent results.2
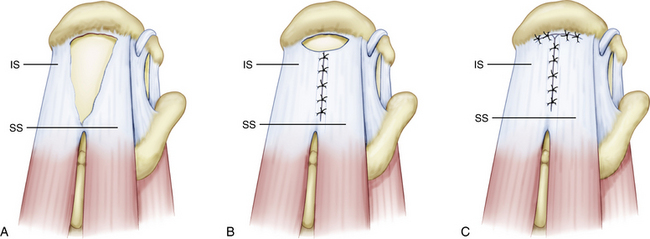
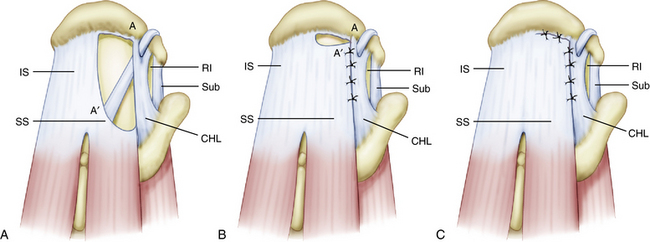
In the fourth tear pattern, the massive, contracted, immobile rotator cuff tear, other techniques must be used.
HISTORY AND PHYSICAL EXAMINATION
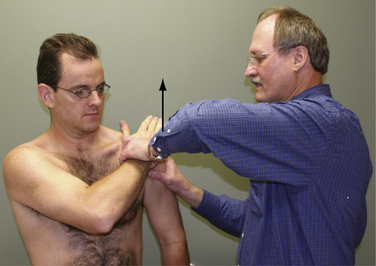
The subscapularis examination is a key element to the shoulder examination that is frequently untested. The lift-off test is not positive until at least 75% of the subscapularis tendon is detached and therefore is not a good test for upper subscapularis tears.18 The bear hug test is the most sensitive test for a torn subscapularis, particularly a partial tear involving only the upper subscapularis.19 In this test, the patient places the hand of the affected side on the opposite shoulder with the fingers extended and the elbow elevated into a forward position. The examiner then tries to pull the patient’s hand off the shoulder perpendicular to the plane of the forearm as the patient resists (Fig. 21-7). If the examiner is able to lift the patient’s hand off the shoulder, this is a positive finding and is suggestive of at least a partially torn subscapularis tendon. Other tests for the subscapularis include the belly press and Napoleon tests.20
INDICATIONS AND CONTRAINDICATIONS
Traditionally, fatty infiltration of more than 50% on preoperative MRI scans has been considered a poor prognostic indicator for rotator cuff repairs.22–24 These patients have been discouraged from undergoing cuff repair with the assumption that surgical repair would not improve their outcome. In the senior author’s practice (SB), assessment of fatty infiltration within the muscle belly of the infraspinatus is critical, because it affects outcome. Muscle imparts elasticity to the rotator cuff and, without adequate muscle tissue, it would be difficult, if not impossible, to repair the tendon to the greater tuberosity. Lo and Burkhart have reported the results of repair of massive immobile rotator cuff tears that required the interval slide technique.21 Their patients demonstrated significant improvements in pain, active forward elevation, active external rotation, strength, and function. More recently, Burkhart and coworkers13 have evaluated the outcomes of massive cuff repairs and correlated these outcomes to preoperative MRI findings. The data suggest that patients who have greater than 75% fatty infiltration have a guarded prognosis for significant improvement because only 40% of these patients demonstrated clinical improvement. This is essential to determine prior to surgery because these patients can then be informed of their less favorable prognosis. They may choose not to proceed with surgical intervention, given their limited probability of functional improvement. However, patients with 50% to 75% fatty infiltration actually improved significantly after rotator cuff repair. In fact, 100% (17/17) of patients with less than 75% fatty infiltration had significant clinical and functional improvement after rotator cuff repair. Thus, in contradistinction to Goutallier’s cutoff of 50%, we consider all patients with less than 75% fatty infiltration on MRI scans to be potential surgical candidates.13
One area in which massive contracted rotator cuff tears are frequently encountered is during revision rotator cuff repair. Many authors have reported the results of revision rotator cuff surgery done through an open approach.1,9,10,22 Overall, these studies have demonstrated that although frequently effective in terms of pain relief, functional improvements have been slight. Recently, Lo and colleagues3 have reported on the arthroscopic revision of failed rotator cuff tears and demonstrated significant functional improvement in 93% of these patients, with a mean increase in the UCLA score of 15.5.
Some authors have also suggested proximal migration as a poor prognostic sign for rotator cuff surgery.23,24 Burkhart and associates18 have demonstrated results to the contrary. In their study of patients who had proximal migration of the humeral head associated with anterosuperior cuff tears (subscapularis plus supraspinatus ± infraspinatus), 80% of patients demonstrated lasting reversal of the superior humeral head migration and a return of overhead function after repair. Proximal migration of the humeral head is not a contraindication to rotator cuff repair. Instead, one could argue that patients with proximal migration of the humeral head have the most to gain from rotator cuff repair. It is important to note, however, in the senior author’s (SB) experience, that proximal migration of the humerus combined with radiographic findings of a rounded greater tuberosity and acetabularization of the acromion suggest a long-standing tear that may be irreparable. In these situations, arthroscopic surgery may have limited applications.




