(1)
Paediatric and Young Adult Orthopaedic Unit, The Royal London and Barts and The London Children’s Hospitals, Barts Health, London, UK
Keywords
AsymmetryFeetHipJointPositionFemurIntroduction
Many children who are brought to paediatric orthopaedic clinics do not have a pathological condition. Some are simply demonstrating natural variation of appearance, with any measured parameter falling within two standard deviations of the mean. Others may be manifesting either features of a natural developmental process (e.g. bow legs) or minor variations that are likely to correct spontaneously with further growth and development (e.g. persistent femoral anteversion).
Bow Legs
The majority of infants are bow-legged before they stand and walk. It is common for this tendency to persist when the child first starts to bear weight, and the tendency is more marked in early walkers. This bow leg, or genu varum, is characterised by its bilateral and generally symmetrical nature, and the bowing is usually more apparent in the femoral segment than in the tibial segment (Fig. 1.1). The degree of varus is often seen to increase during the first 6–12 months after standing, before it gradually improves spontaneously between the ages of 2–3 years. This so-called physiological genu varum requires only a clear explanation and reassurance to the parents, and no treatment is needed. Asymmetry, associated torsional problems, and varus which continues to increase beyond the age of 2 years may be pathological rather than a normal variant; the possibility of Blount’s disease or rickets should be considered, and radiographs and blood profile for vitamin D deficiency should be obtained.
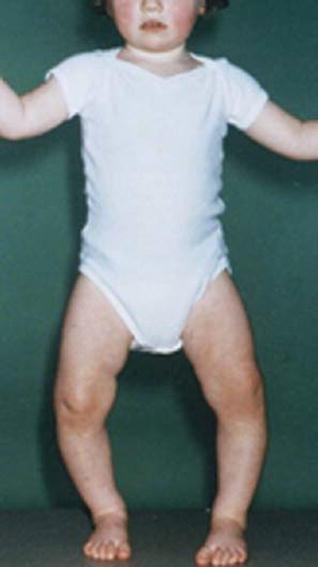
Figure 1.1
Bow legs (Reproduced from Benson et al. Children’s Orthopaedics and Fractures, 2009, Springer)
Otherwise, regular clinical review with estimation of the intercondylar distance at the knees should be undertaken until it is clear that the normal process of spontaneous resolution is occurring.
Spontaneous resolution occurs through differential stimulation of the medial and lateral areas of the distal femoral and proximal tibial growth plates by weight-bearing compressive stresses. Sometimes the compensatory growth stimulation is excessive and parents need to be warned that following the straightening of the bowing, there may be a period of overcompensation into valgus or knock-knee before the legs finally straighten out to around 5–7° of valgus by the age of 4–5 years (Fig. 1.2).
Figure 1.2
Normal development of the tibio-femoral angle in children (Data from Baratz M, Watson AD, Imbriglia JE. Orthopaedic Surgery the Essentials. Thieme, 1999)
Knock-Knees
Genu valgum or knock-knee (Fig. 1.3) may be a result of overcompensation following a period of genu varum (see above), or it may be a feature of generalised joint laxity (benign hypermobility) particularly in a heavy child. In this latter instance, it may be associated with postural flat feet. Again, if the condition is symmetrical and there is no evidence of vitamin D deficiency, no treatment is required as spontaneous improvement is likely. Regular monitoring of the intermalleolar distance with the child lying on the couch removes the effect of ligamentous laxity, and is an acceptable assessment of progress. Occasionally the knock-knee will persist beyond the first few years of life, and if greater than 12–15° in the older child, may warrant correction by guided growth techniques (hemiephysiodesis).





