but scored at 4). MRI is also scored at 9 if radiographs are suspicious for malignancy with CT scored at 5 and FDG-PET imaging also scored at 5.10 CT is still recommended if osteoid osteoma is suspected (scored 9 with bone scans as an alternative and scored 6 of 9).10
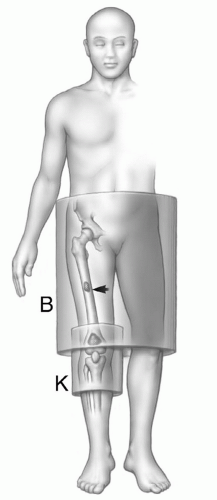 Figure 12.1 Illustration of a primary sarcoma in the knee with a mid femoral skip lesion. The knee coil would be optimal for imaging the knee, but the skip lesion cannot be identified unless the entire femur is examined. |
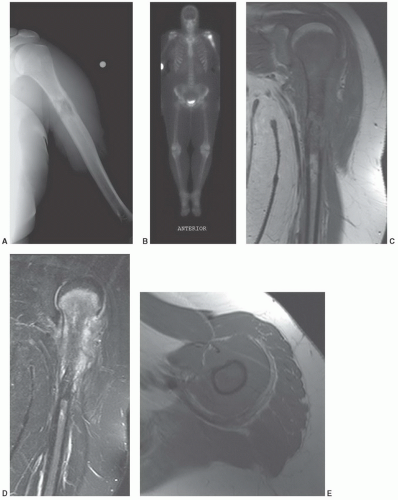 Figure 12.2 High-grade osteosarcoma. A: Radiograph demonstrates a destructive lesion in the upper humerus with periosteal reaction. B: Technetium-99m MDP whole body bone scan demonstrates intense uptake in the proximal humerus with no distant metastasis. Coronal T1- (C) and STIR (D) images and axial T1-weighted (E), T2-weighted (F), and postcontrast (G) images clearly demonstrate the extent of the tumor. H: Specimen radiograph of the resected proximal humerus. Note the significant (>5 cm) margin of normal bone adjacent to the distal tumor extent. I: The patient was treated with a long stem hemi-arthroplasty component and proximal allograft with cortical bone graft at the allograft-humeral junction. (From Berquist TH. Imaging of Orthopedic Fixation Devices and Prostheses. Philadelphia: Lippincott-Williams and Wilkins; 2009.) |
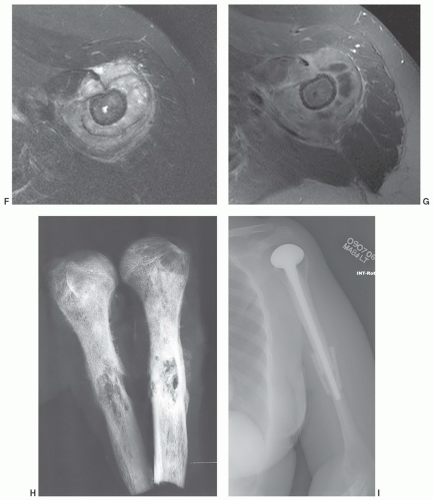 Figure 12.2 (continued) |
additional imaging plane or planes will vary with the involved body part, the lesion location, and its relationship to crucial structures. In general, the additional plane is sagittal with anterior or posterior masses and coronal with medial or lateral lesions. Oblique planes may also be a useful adjunct to reduce the problems from partial volume effects (Figs. 12.4 and 12.5). In these additional planes, a combination of conventional T1- and T2-weighted spin-echo (SE) images, turbo (fast) spin-echo images, gradient images, and STIR imaging is useful, as the cases require.
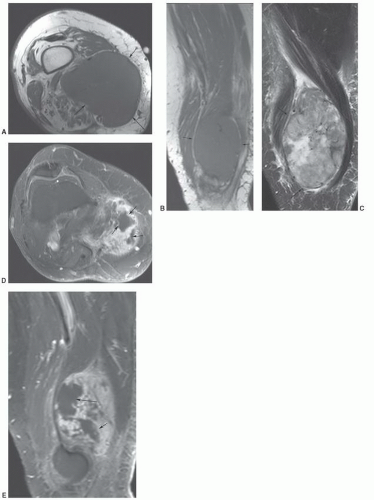 Figure 12.3 High-grade leiomyosarcoma. Axial (A) and sagittal (B) T1-weighted and sagittal turbo spin-echo T2-weighted sequences demonstrate a large soft tissue mass (arrows) with inhomogeneous signal intensity on the T2-weighted sequence (C). Axial (D) and sagittal (E) post-contrast fat suppressed T1-weighted images demonstrate areas of non-enhancement (arrows) due to tissue necrosis. |
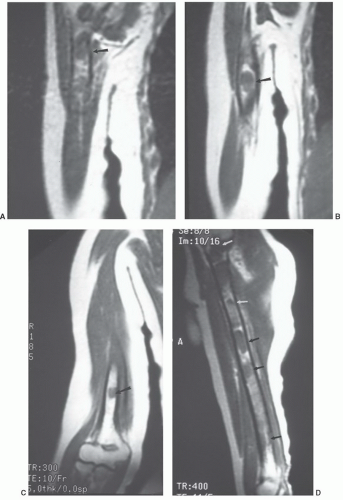 Figure 12.4 Middle-aged man with lymphoma and arm pain. A phased array coil was used to evaluate the right humerus. Coronal T1-weighted images (A-C) do not include the entire structure on a single image plane. Diffuse involvement (arrows) is apparent when a sagittal image (D), which shows the entire length of the humerus, is selected. |
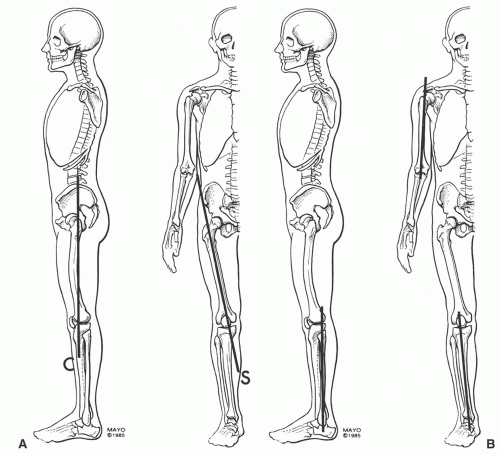 Figure 12.5 Skeletal illustrations demonstrating oblique planes required to accurately access the long bones. A: The femur is most easily evaluated in the oblique sagittal plane (S) due to the normal anterior bowing, which creates partial volume problems in the coronal plane (C). B: The oblique sagittal plane is also most useful for the humerus. Either the sagittal or the coronal plane can be used for the tibia and fibula. |
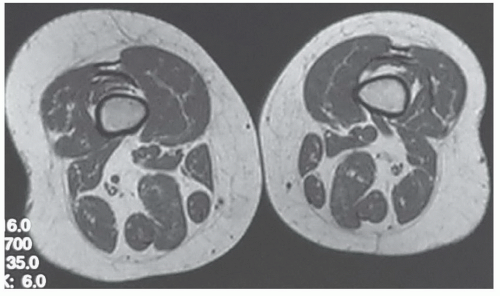 Figure 12.6 Lipomatosis of the right lower extremity in a 54-year-old woman presenting with “fullness” around the knee. Axial T1-weighted MR image of both distal thighs shows increased adipose tissue on right as compared with contralateral side. Images of both distal thighs were obtained after no cause for clinical findings was found on axial images of right knee. |
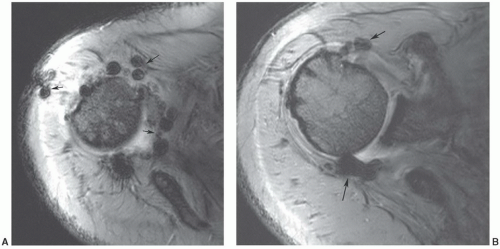 Figure 12.7 Gradient-echo axial images of the shoulder (A and B) following rotator cuff repair. There are multiple blooming artifacts (arrows) due to metal debris. |
malignant lesions.30,32 Dynamic studies using fast scan techniques were initially reported by Erlemann et al.27,28 Others have also studied these techniques, but with inconsistent results. In our practice, we reserve the use of dynamic gadolinium studies for selected cases (see below, limitations of MRI) (Figs. 12.8 and 12.9).
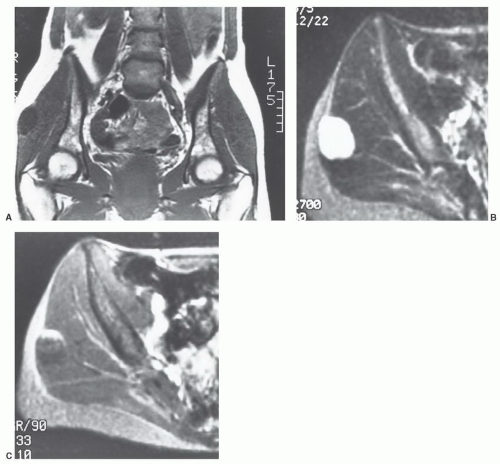 Figure 12.8 Myxoma. Coronal T1-weighted (A) and axial T2-weighted (B) images demonstrate a well-defined lesion with low intensity on T1-weighted (A) and high uniform signal intensity on T2-weighted (B) images. These features are characteristic of myxoma. After gadolinium injection (C), the enhancement pattern is inhomogeneous and nonspecific. |
MR images will show the changes associated with the foreign body, although the foreign body itself may have no signal and may be difficult to identify. We have found ultrasound a useful adjunct in such cases (Fig. 12.10).40
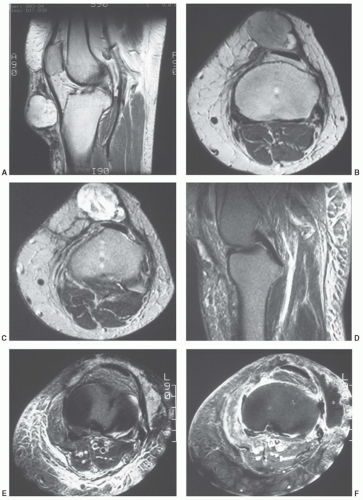 Figure 12.9 Sagittal T2-weighted (A), axial proton density-weighted (B) and T2-weighted (C) images demonstrate an inhomogeneous lesion in the anterior knee. The lesion was surgically removed and was found to be a high-grade pleomorphic sarcoma. Sagittal (D) and axial (E) T2-weighted images 1 year later show an area of increased signal intensity (asterisk) anterolaterally. There is a large amount of edema due to radiation therapy. Post-gadolinium image (F) shows peripheral enhancement with low intensity in the region of interest (asterisk) indicating a fluid collection and not a solid mass. |
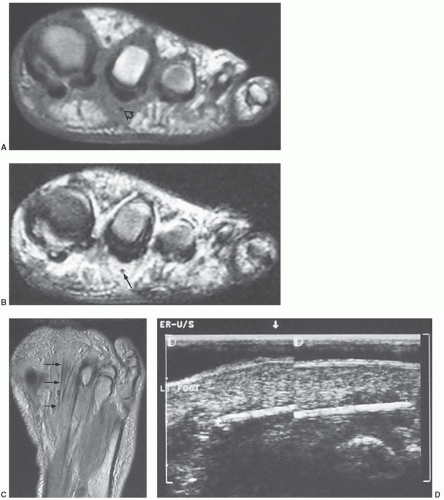 Figure 12.10 Toothpick foreign body in the foot of a 49-year-old woman. Coronal T1- (A) and T2-weighted (B) MR images show poorly defined abnormal signal intensity with a small mass below the second toe. The small signal void within the mass is the toothpick foreign body (arrow). C: Axial proton density-weighted MR image shows the foreign body as a linear signal void (arrows). D: Follow-up ultrasound shows the toothpick to better advantage. |
Table 12.1 Enneking System: Staging of Musculoskeletal Neoplasms | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||
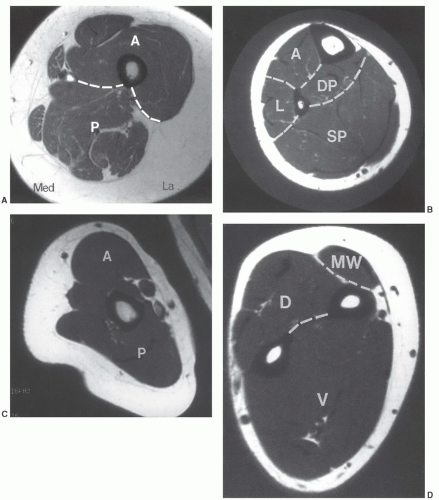 Figure 12.11 Compartmental anatomy. A: Thigh divided into anterior (A), posterior (P), and medial compartments. The anterior compartment contains the quadriceps and sartorius muscles; the posterior compartment contains the semimembranosus, semitendinosus, and biceps group; and the medial compartment contains the adductors and gracilis muscles. B: The calf is divided into, anterior (A), lateral (L), superficial posterior (SP), and deep posterior (DP) compartments. The anterior compartment contains the extensors hallucis longus and digitorum longus and the tibialis anterior. The lateral compartment contains the peroneus brevis and longus. The superficial posterior compartment contains the gastrocnemius and soleus and the deep posterior compartment comprises the tibialis posterior, flexor hallucis longus, and flexor digitorum longus. C: The arm is divided into anterior (A) and posterior (P) compartments. The anterior compartment contains the biceps brachii and brachialis and the posterior compartment the triceps. D: The forearm is divided into the volar (V), dorsal (D), and mobile wad (MW). The volar compartment contains the flexor muscle groups, pronator teres, and palmaris longus, and the dorsal compartment contains the extensor muscle groups and abductor pollicis longus. The mobile wad contains the brachioradialis and extensor carpi radialis longus and brevis. (From Berquist TH. Imaging of Orthopedic Fixation Devices and Prostheses. Philadelphia: Lippincott-Williams and Wilkins; 2009.) |
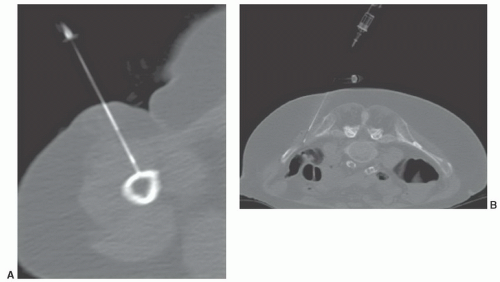 Figure 12.12 Needle biopsy. CT-guided needle biopsies of the humerus (A) in a patient with lymphoma. The needle enters through the anterior compartment. CT-guided biopsy (B) of an iliac lesion entering posteromedially. (From Berquist TH. Imaging of Orthopedic Fixation Devices and Prostheses. Philadelphia: Lippincott-Williams and Wilkins; 2009.) |
| ||||||||||||||||||||||||||||||||||||
MRIis the technique of choice for detection and local staging of soft tissue lesions. Certain benign lesions, such as lipomas, myxomas, hemangiomas, and cysts have characteristic appearances that may obviate the need for biopsy or surgical intervention (Fig. 12.13). Malignant or indeterminate lesions are evaluated using T1- and T2-weighted conventional or fast spin-echo sequences with or without fat suppression. Gadolinium-enhanced T1-weighted images are also obtained. Two image planes are necessary to fully evaluate the extent, compartment, and neurovascular involvement (Fig. 12.3). Dynamic gadolinium techniques may be of value for differentiating benign form malignant lesions. Angiography is not often performed, but can be used for indications noted above.
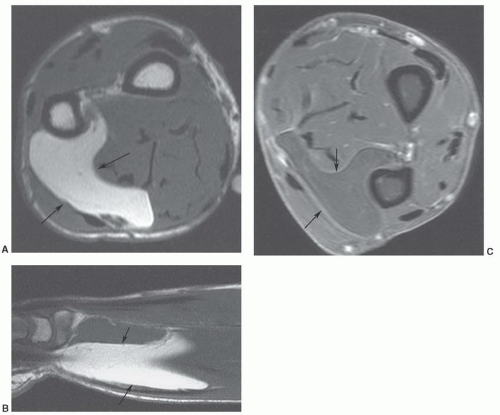 Figure 12.13 Benign lipoma. Axial (A) and sagittal (B) T1-weighted and axial fat-suppressed turbo spin-echo T2-weighted (C) images demonstrate a large fatty tumor in the distal forearm with no signal changes to suggest low-grade malignancy. |
an underlying skeletal deformity (such as exuberant callus related to prior trauma) or bony exostosis that may masquerade as a soft tissue mass. Radiographs may also reveal the presence and nature of soft tissue calcifications, which can be suggestive and at times very characteristic of a specific diagnosis. For example, they may reveal the phleboliths within a hemangioma, the juxta-articular osteocartilaginous masses of synovial osteochondromatosis, the peripherally more mature ossification of myositis ossificans, or the characteristic bone changes of other processes with associated soft tissue involvement (Fig. 12.15).
| ||||||||||||||||||||||||||||||||||
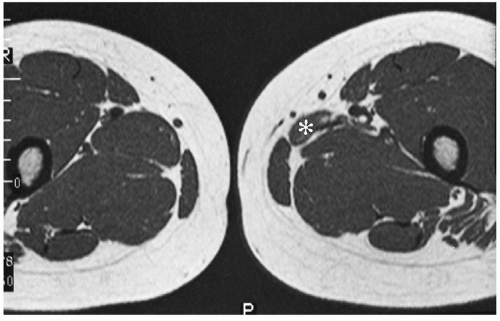 Figure 12.14 Atrophied adductor muscle in a 24-year-old woman presenting with soft tissue asymmetry, suggesting a soft tissue mass. Axial T1-weighted MR image shows the marked atrophy to the left adductor longus muscle (asterisk). Atrophy was secondary to a previous muscle injury. |
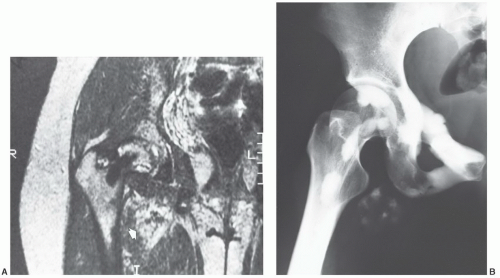 Figure 12.15 Melorheostosis in a 26-year-old woman presenting with hip pain and a soft tissue mass in the right groin. A: Coronal T2-weighted MR image of the hip shows a heterogeneous nonspecific soft tissue mass (arrow). The lesion showed signal intensity similar to that of skeletal muscle on corresponding T1-weighted image (not shown). An associated interosseous abnormality is noted in the proximal femur. B: Corresponding radiograph readily confirms the diagnosis of melorheostosis with soft tissue involvement. |
of pulse sequence (Fig. 12.17).59,60,61,62,70 When significant fibrous tissue is present, these lesions may be termed fibrolipomas. It is important to remember that when a fatty lesion does not meet the imaging requirements for a lipoma, liposarcoma is typically the diagnosis of exclusion; however, lipoma variants are encountered more commonly than liposarcoma.59,71
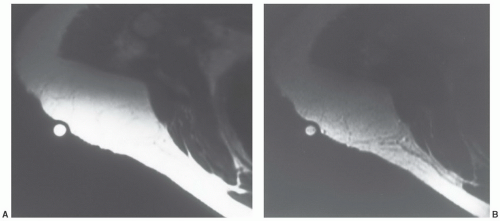 Figure 12.16 Superficial lipoma in the subcutaneous tissue of the shoulder of a 65-year-old woman. A: Axial T1-weighted MR image of the right shoulder shows a poorly defined mass, imaging identical to that of subcutaneous fat. Such lesions may be inapparent on MRI unless a marker is placed over the palpable abnormality. B: Corresponding non-fat suppressed T2-weighted MR also shows the lesion to image identical to that of subcutaneous fat. |
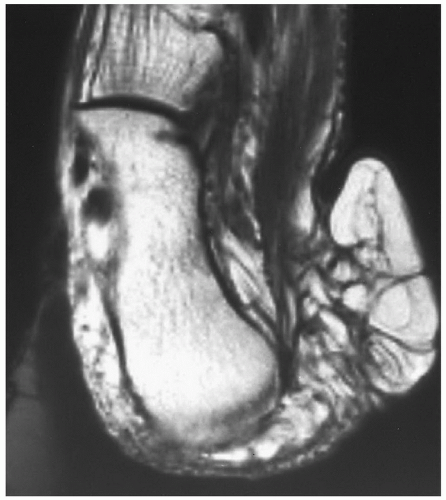 Figure 12.17 Recurrent superficial lipoma in the subcutaneous tissue of the heel in a 69-year-old woman. T1-weighted MR image shows the mass to have a lobulated contour with signal intensity identical to that of subcutaneous fat. The lesion has multiple linear septations of decreased signal intensity coursing through its substance. These showed similar decreased signal intensity on T2-weighted images (not shown). They corresponded to fibrous tissue on histologic examination. Lesions such as these are often referred to as fibrolipoma. |
tissues; however, involvement isolated to the intermuscular region (intermuscular lipoma) is less common. Intramuscular lipoma occurs in patients of all ages but predominantly in adults, with most cases presenting in patients between 30 and 60 years of age.52 There is a slight male predominance. Patients typically present with a mass in the large muscles of the extremities, especially the thigh, shoulder, and upper arm. The fat within the intramuscular lipoma may infiltrate between skeletal muscle fibers, giving the intramuscular lipoma a striated appearance on gross inspection.
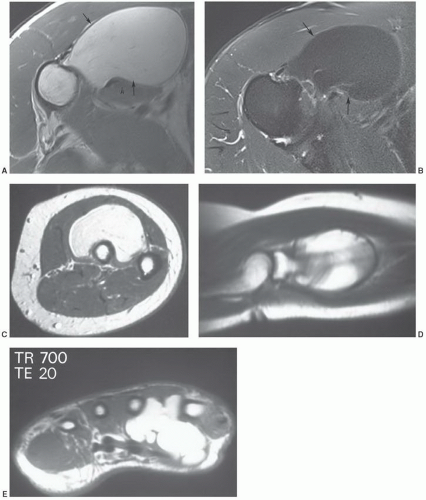 Figure 12.18 Benign lipomas, multiple patients. Axial T1-weighted (A) and T2-weighted (B) images of a benign lipoma along the proximal humerus with (arrows). C and D: Axial and sagittal T1-weighted images of a benign lipoma in the supinator muscle. E: Axial T1-weighted MR image of a lobulated lipoma in the hand. |
MRI as a predominantly fatty mass (with signal intensity equal to that of the subcutaneous fat), infiltrating the adjacent skeletal muscle. The mass is usually well defined and sharply circumscribed, with imaging characteristics similar to that of an “ordinary lipoma.” This lesion has also been referred to as “infiltrating lipoma.” Despite being well-defined radiologically, margins are frequently infiltrating at microscopy, with adipose tissue intermingled with skeletal muscle fibers that are variably atrophic (Figs. 12.20 and 12.21). Matsumoto et al.75 reported the MR appearance of intramuscular lipoma in 17 cases and found the lesion to be homogeneously pure fatty tissue in 12 (71%), with the remainder being fat with intermingled muscle fibers, the latter showing a signal intensity identical to that of skeletal muscle on T1- and T2-weighted pulse sequences. An infiltrative margin was seen in 7 cases (41%).
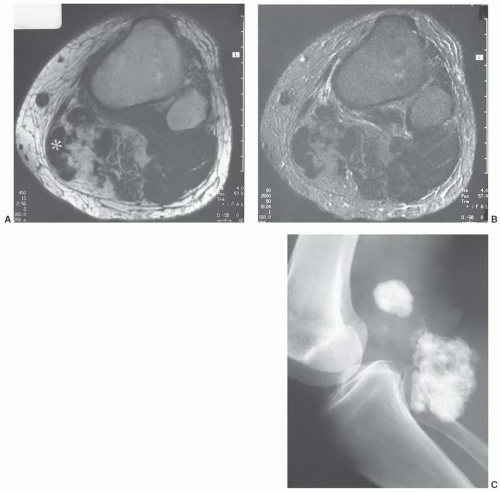 Figure 12.19 Benign mesenchymoma in the popliteal fossa of a 79-year-old man. A: Axial T1-weighted MR image shows a fatty mass with a central region of markedly decreased signal intensity (asterisk). B: Corresponding T2-weighted image shows similar findings. C: Radiograph shows densely mineralized mass. |
and foot. Lipoma arborescens usually involves the knee.60,76 About 20% of the time, knee involvement is bilateral.77
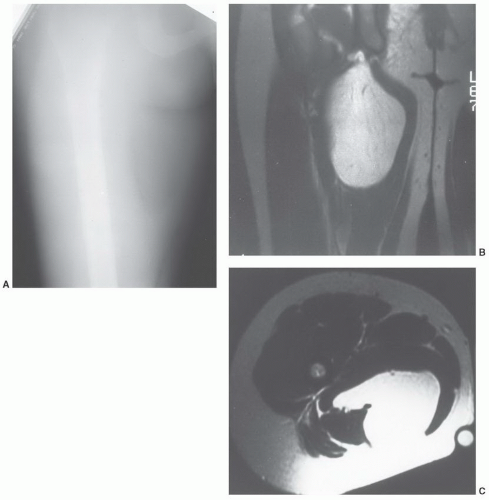 Figure 12.20 Intramuscular lipoma in the thigh of a 29-year-old woman. A: Anteroposterior radiograph shows a fat density mass in the medial aspect of the proximal right thigh. B: Corresponding coronal T1-weighted MR image shows the signal intensity of the mass to be identical to that of the subcutaneous fat. C: Axial T1-weighted localizes the mass to the adductor compartment. |
hamartoma of nerve, perineural lipoma, fatty infiltration of the nerve, and intraneural lipoma.80,81 The term “neural fibrolipoma” was originally preferred because it better describes the underlying pathology.80 More recently, the WHO has adopted the term lipomatosis of nerve.62 The cause of this disorder remains unclear; it may be related to hypertrophy of mature fat and fibroblasts in the epineurium.81
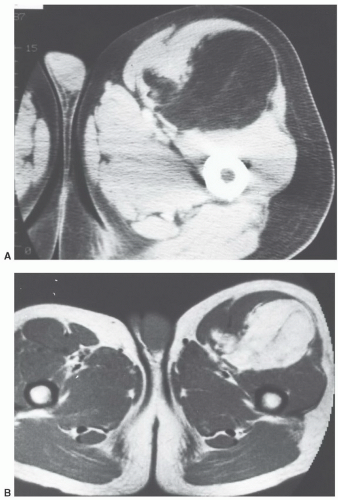 Figure 12.21 Intramuscular lipoma in the thigh of a 50-year-old man. A: Axial CT shows a fatty mass in the anterior aspect of the left thigh. There are some small areas of increased attenuation within the lesion. B: Corresponding axial T1-weighted MR image nicely shows the fatty nature of the mass. The area of increased attenuation on CT on the medial aspect of the mass images is identical to skeletal muscle and is compatible with muscle infiltrating the margin of the lesion. Similar findings were seen on T2-weighted images (not shown). |
appearing as a tan yellow mass within the nerve sheath.84 Microscopy demonstrates infiltration of the epineurium and perineurium by fibrofatty tissue.81 Cases in which there is macrodactyly are histologically indistinguishable from those in which there is no macrodactyly.81
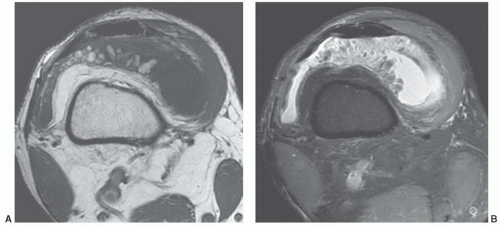 Figure 12.22 Lipoma arborescens in a 58-year-old man. Axial T1-weighted (A) and T2-weighted (B) MR images show a joint effusion with fat in a frond-like pattern, representing the synovial villi, distended with adipocytes. |
mass.86 The adjacent bone may demonstrate solid periosteal reaction, cortical thickening, saucerization, or osseous excrescences.68,91 Osseous changes are seen in 67% to 100% of cases,68,91,92 although these may be subtle. The periosteal reaction in two cases reported by Murphey et al.91 was minimal, being identified only on magnification radiography. The osseous excrescences do not demonstrate the cortical and medullary continuity or hyaline cartilaginous cap seen with a true osteochondroma.68
 Figure 12.23 Macrodystrophia lipomatosa. A: Radiograph of the hand demonstrates abnormalities of both bone and soft tissue. The phalanges are long, broad, and splayed at their distal ends. The osseous overgrowth is marked and disproportionately large with extensive secondary degenerative change. Coronal (B) and Axial (C) MR images in a different patient demonstrating fatty change in the finger and a neural fibrolipoma of the median nerve in (C). |
that adult cases represent delayed presentation. Diffuse lipomatosis typically affects the limbs, although involvement of the trunk and chest wall may be seen.93 Lipomatosis may be associated with coexistent osseous hypertrophy, but unlike macrodystrophia lipomatosa, the nerve is unaffectedand the disease is not confined to an extremity. Reported as rare,52 we believe that mild cases of lipomatosis are not uncommon and may be easily overlooked (Fig. 12.6).
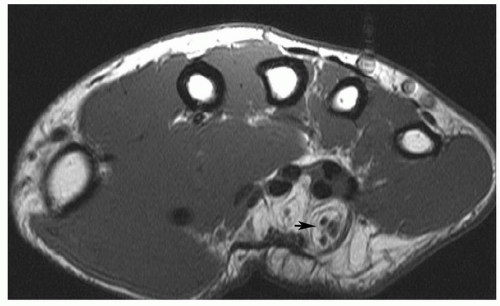 Figure 12.24 Neural fibrolipoma. Axial T1-weighted image of the wrist demonstrating a fibrolipoma of the ulnar nerve (arrow). |
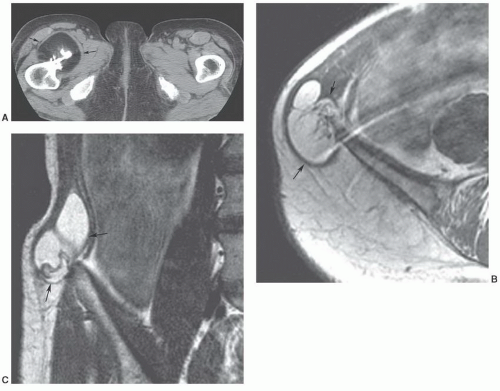 Figure 12.25 Parosteal lipomas. A: Axial CT of a parosteal lipoma of the upper femur (arrow). Axial (B) and coronal (C) T1-weighted images in a different patient demonstrating a parosteal lipoma of the ilium (arrows). |
recurrence and metastasis. While the round cell liposarcoma was previously identified as distinct subtypes by the WHO Classification of Soft Tissue Tumors, the myxoid and round-cell liposarcoma are now combined under the designation of myxoid liposarcoma.62 These lesions were known to form a histological continuum, and represented the ends of a common spectrum.58 Now under a single diagnosis, the pure myxoid lesion is considered an intermediate grade tumor at the low-grade end of this spectrum, while the hypercellular (round cell) morphology represents the histologically similar, high-grade counterpart. The presence of the hypercellular component is associated with a more aggressive clinical course and a significantly worse prognosis.95 Well-differentiated liposarcomas are most common, accounting for about 54% of all classified liposarcomas. Myxoid liposarcoma is next most common,
accounting for 28%, followed by dedifferentiated (10%), and pleomorphic liposarcomas.96 Liposarcomas tend to occur in both the retroperitoneum and extremities, with extremity lesions presenting about 10 years earlier than those in the retroperitoneum. Dedifferentiated liposarcomas are most common in the retroperitoneum, whereas the other subtypes are more common in the extremities.96
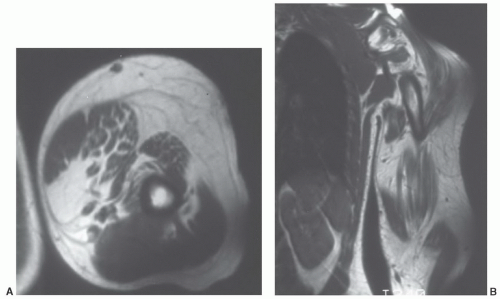 Figure 12.26 Upper extremity lipomatosis in a 23-year-old man. Axial (A) and coronal (B) T1-weighted SE MR images of the left upper extremity show diffuse overgrowth of adipose tissue. |
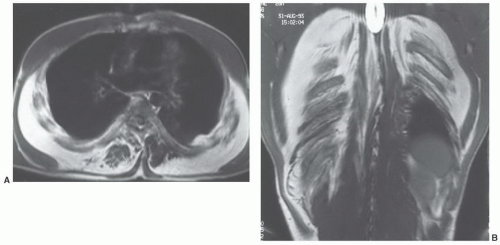 Figure 12.27 Symmetric lipomatosis in a 28-year-old man. Axial (A) and coronal (B) T1-weighted MR images show extensive, but symmetric, lipomatosis of the chest wall. |
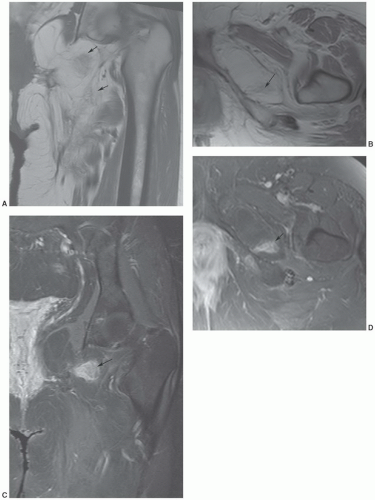 Figure 12.28 Well-differentiated liposarcoma of the left groin and upper thigh. Coronal (A) and axial (B) T1-weighted images demonstrate a fatty tumor with globular areas of low signal intensity (arrows). Coronal (C) and axial (D) T2-weighted images demonstrate corresponding areas of high signal intensity (arrows). |
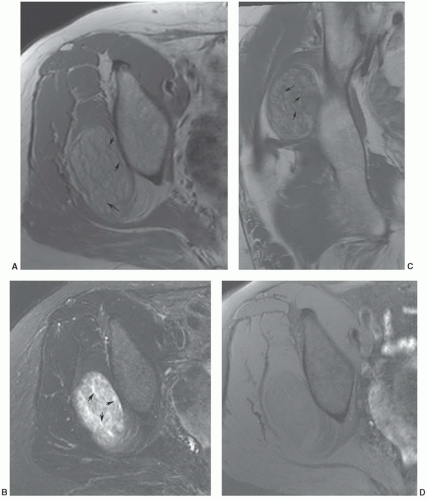 Figure 12.29 Well-differentiated gluteal liposarcoma. Axial T1- (A) and T2-weighted (B) images demonstrate a well defined (<10 cm) lesion with thickened septa (arrows). Coronal T1-weighted image (C) demonstrates similar findings (arrows). Post-contrast fat-suppressed T1-weighed image (C) shows no enhancement. |
from a well-differentiated liposarcoma, lipoma variants occur with an imaging appearance that will overlap that of a well-differentiated liposarcoma. The distinction of lipoma and well-differentiated liposarcoma is simple when the former is homogeneous with an imaging appearance identical to that of the subcutaneous adipose tissue. When nonadipose elements are present, however, this distinction may be quite problematic. Recent literature has documented awider spectrum for the imaging features of lipoma than had been previously appreciated, with a small but significant number of lipomas demonstrating prominent nonadipose areas and an imaging and appearance that may mimic that traditionally ascribed to well-differentiated liposarcoma.96 In these cases, the nonadipose areas represent fat necrosis and associated calcification, fibrosis, inflammation, and myxoid change. As a generalization, lesion size may also be useful, in that well-differentiated liposarcoma tends to be significantly larger than lipoma. In a recent review of 60 well-differentiated fatty tumors, the average largest dimension of malignant lesions was nearly twice that of benign lipomas (24 cm vs. 13 cm).96 Enhancement pattern may also be useful, with well-differentiated tumors showing contrast enhancement.98 Kransdorf et al.,61 noted that statistically significant features of liposarcoma included lesions more than 10 cm in size (p <.001), thick septa (p = .001), lesion less than 75% fatty tissue (p <.001), and globular or nodular areas of non-fatty tissue.61
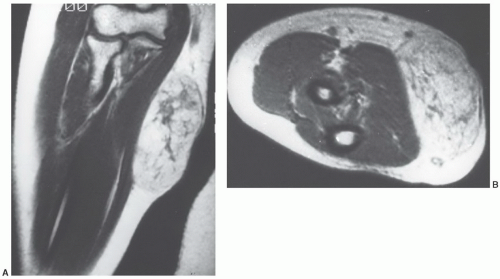 Figure 12.30 Well-differentiated liposarcoma of the upper extremity in a 34-year-old woman. A: Coronal T1-weighted MR image of the forearm shows a fatty subcutaneous mass. The mass is predominantly fatty but shows linear and globular areas of non-fatty tissue within it. B: Axial T2-weighted image shows linear areas of non-fatty tissue, although these are not as conspicuous as those seen in A. This is the type of lesion sometimes referred to as an atypical lipoma. |
histologically indistinguishable, and the term “atypical lipoma” has been advocated by some to spare the patient a malignant diagnosis and prevent unnecessary radical surgery for well-differentiated lipomatous tumors of the extremity. However, other investigators prefer the term “well-differentiated liposarcoma” for deep fatty tumors of the extremities because of the propensity of these tumors to recur and because of the remote possibility of dedifferentiation; either de novo or in recurrences. One could theoretically categorize both atypical lipoma and well-differentiated liposarcoma as atypical lipomatous tumors, because both have a propensity to recur locally but no tendency to metastasize.99 Lesions with similar histology in the retroperitoneum have retained the designation of well-differentiated liposarcoma because of their association with multiple local recurrences (presumably because they are frequently incompletely resected) and because such lesions may eventually be fatal.102,103,104,105
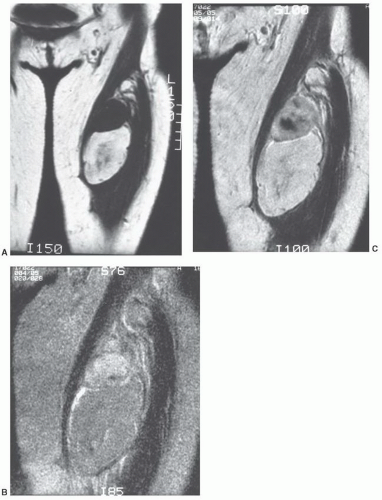 Figure 12.31 Recurrent dedifferentiated liposarcoma in the thigh of a 33-year-old woman. A: Coronal T1-weighted image shows a mass in the anterior left thigh. The well-differentiated portion of the mass images similarly to subcutaneous fat. B: Corresponding T2-weighted image shows the non-fatty component to have signal intensity higher than that of fat. Note areas of increased signal intensity in well-differentiated portion. C: Gd-DTPA-enhanced T1-weighted (650/20) image shows significant enhancement in the high-grade component and mild enhancement within the well-differentiated portion of the tumor. (From Kransdorf MJ, Meis JM, Jelinek JS. Dedifferentiated liposarcoma of the extremities: imaging findings in 4 patients. AJR Am J Roentgenol. 1993;161:127-130, with permission.) |
lesions in the deep somatic soft tissues, we would agree with Weiss and Goldblum and use the term “atypical lipoma” only for subcutaneous extremity lesions, reserving the term “well-differentiated liposarcoma” for lesions with similar histologies in all remaining sites.52,58
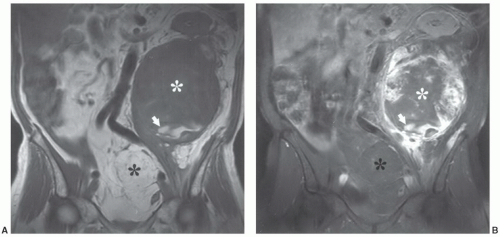 Figure 12.32 Dedifferentiated liposarcoma in the retroperitoneum of a 74-year-old man. Coronal T1-weighted (A) and postcontrast fat-suppressed coronal T1-weighted (B) images show a large mass (white asterisk) with a juxtaposed poorly defined predominantly non-fatty component (black asterisk) (fat much less than 25% of the lesion). Note central nonenhancing area in B (asterisk). Area of high signal intensity inferiorly (arrow) represents subacute blood, in keeping with previous hemorrhage and necrosis. Also note superior displacement of kidney. |
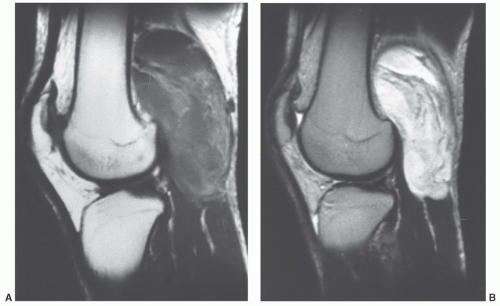 Figure 12.33 Myxoid liposarcoma in the popliteal fossa of a 22-year-old man. Sagittal T1-weighted (A) and T2-weighted (B) images show thickened linear and amorphous fatty areas within an otherwise nonspecific mass. |
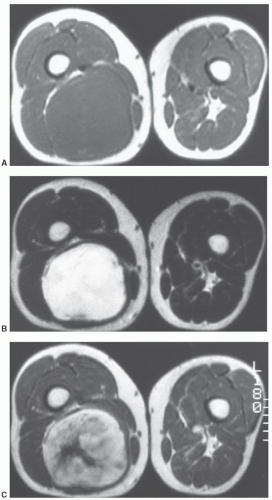 Figure 12.34 Myxoid liposarcoma in the posterior thigh of a 49-year-old man. Axial T1-weighted (A) and T2-weighted (B) images show a nonspecific mass in the posterior right thigh. C: Corresponding nonfat suppressed T1-weighted image after Gd-DTPA administration shows marked enhancement. |
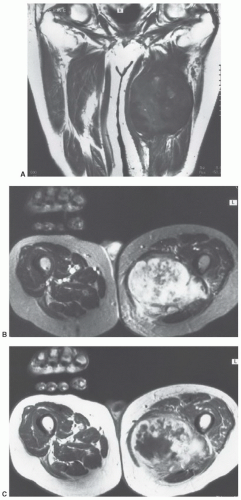 Figure 12.35 Pleomorphic liposarcoma in the posterior thigh of an 85-year-old man. A: Coronal T1-weighted image shows a large predominantly non-fatty inhomogeneous mass with central areas of increased signal intensity. B: Axial T2-weighted image is very inhomogeneous, but otherwise nonspecific. C: Corresponding axial T1-weighted non-fat suppressed image after Gd-DTPA administration shows marked irregular peripheral enhancement. |
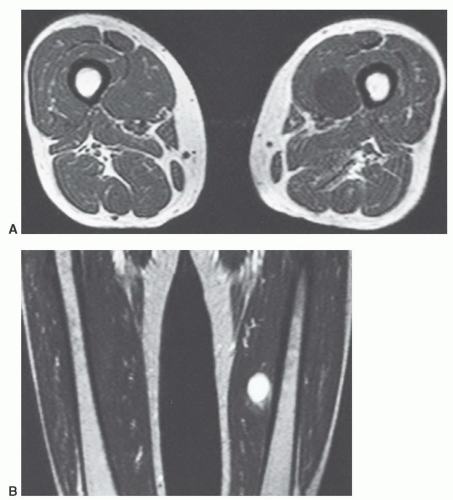 Figure 12.36 Myxoid liposarcoma in the thigh of a 56-year-old woman. Axial T1-weighted (A) and coronal T2-weighted (B) images show a round well-defined lesion in the medial aspect of the left thigh. The lesion has imaging characteristics identical to a cyst or myxoma. |
Weiss authored by Weiss and Goldblum121 have devised a more anatomic approach to benign vascular lesions. The subtypes include synovial hemangiomas arising in the synovium, intramuscular which is a proliferation of benign vessels in muscle, venous hemangiomas, and arteriovenous hemangiomas with shunts and a mix of venous and arterial structures.118,119,120,121 Other categories include the epithelioid hemangioma, a feeding artery, and well-defined mature vessel lined by epithelioid endothelial cells and stroma mimicking lymph nodes.118 Angiomatosis is another category with a diffuse hemangioma affecting large anatomic regions that crosses tissue planes and compartments.118,122
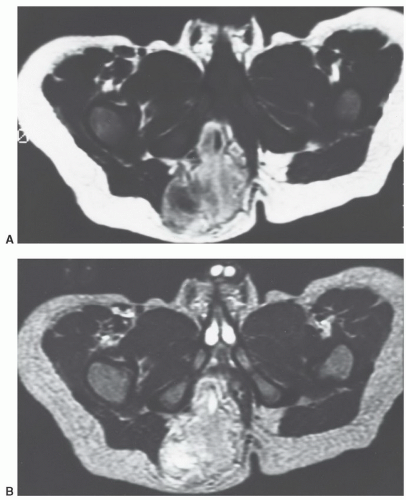 Figure 12.37 Lipoblastoma in a 1-year-old boy. Axial T1- (A) and T2-weighted (B) images show a large predominantly fatty mass with a significant non-fatty component. In an adult, this appearance would suggest a liposarcoma. |
compared with subcutaneous fat (Fig. 12.41).125,128 Segments of the lesion are isointense to either fat and/or muscle. MR angiography is useful for evaluation of the vascular supply of the lesion (Fig. 12.41). Phleboliths (within the hemangioma) may be detected as small rounded areas of signal void on MRI, but these are more readily apparent on radiographs or CT.116 Marrow signal abnormalities may be seen adjacent to large hemangiomas. Although their nature is not known, they are hypothesized to represent either marrow edema or hematopoietic conversion with localized hyperemia.126
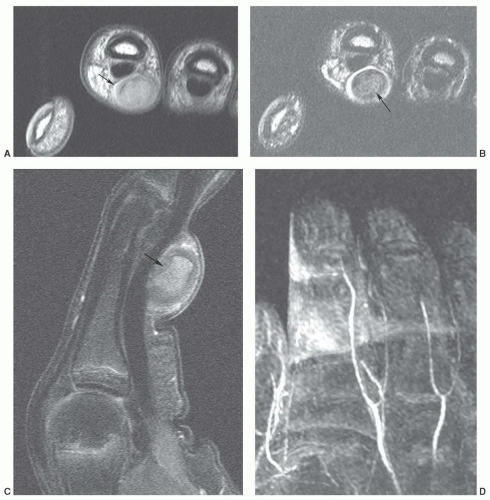 Figure 12.38 Thrombosed superficial hemangioma in the hand. Axial T1-weighted (A) and T2-weighted (B), sagittal fat-suppressed post-contrast T1-weighted (C) and MR angiogram (D) demonstrate the thrombosed hemangioma (arrow) with occlusion of several digital arteries (D). |
 Figure 12.39 Deep intramuscular hemangioma of the forearm. Axial (A) and sagittal (B) T1-weighted and axial (C) and sagittal (D) T2-weighted images demonstrate a large hemangioma in the forearm. |
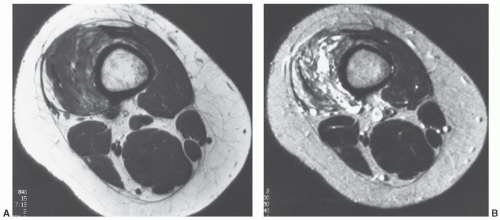 Figure 12.40 Intramuscular hemangioma in the thigh of a 23-year-old woman. A: Axial T1-weighted image shows areas of increased signal, in a lacelike pattern, coursing through the lesion. B: Corresponding axial T2-weighted image shows the lesion to have a lobular configuration with areas markedly hyperintense to subcutaneous fat, and others isointense to fat and skeletal muscle. |
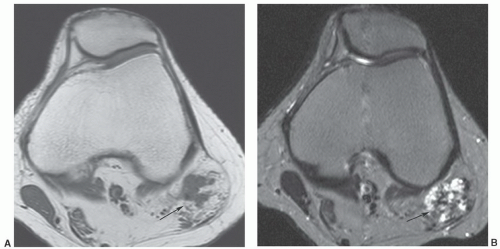 Figure 12.41 Biceps femoris hemangioma. Axial T1-weighted (A) and T2-weighted (B) and sagittal fat-suppressed turbo spin-echo (C) images demonstrate the hemangioma at the myotendinous junction (arrow). MR angiogram (D) clearly demonstrates the vascular supply and lesion vascularity. |
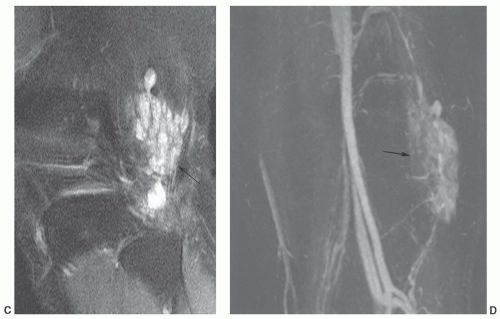 Figure 12.41 (continued) |
of congenital obstruction of lymphatic drainage.138,139 Its progressive nature, however, has suggested that it may be a benign mesenchymal neoplasm.136
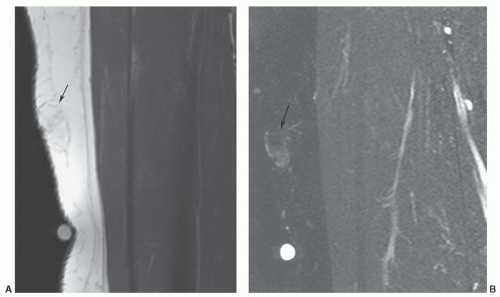 Figure 12.42 Superficial angiolipoma in the thigh. Sagittal T1-weighted (A) and post-contrast fat-suppressed T1-weighted images (B) demonstrate the subtle angiolipoma (arrow). |
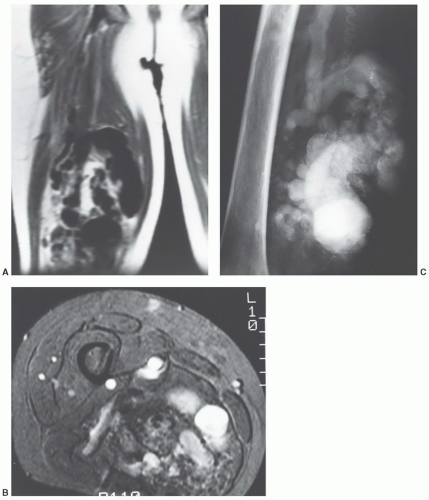 Figure 12.43 Arteriovenous hemangioma (arteriovenous malformation) in the thigh of a 35-year-old man. A: Coronal T1-weighted MR image of the thigh shows prominent flow voids representing rapidly flowing blood in the lesion. B: Axial gradient image shows the lesion to have an infiltrative growth pattern. C: Arteriogram shows the marked vascularity of the lesion, with markedly enlarged, tortuous, draining veins. |
large uniloculated or multiloculated cystic spaces, lined by lymphatic endothelium.136,141 It contains serous or chylous fluid.137 Cystic lymphangiomas are most common in the neck (typically in the posterior cervical space) and axilla, with these locations accounting for 75% and 20% of lesions, respectively.142,143 The prevalence of these locations has been suggested to be the result of sequestered lymphatic anlage, which lack adequate drainage. Other rare locations include the mediastinum, retroperitoneum, bone, omentum, and mesentery.143 Up to 10% of cervical cystic lymphangiomas will extend into the mediastinum.144 Cystic lesions (cystic hygromas) are typically found in regions in which the loose fatty connective tissue allows relatively unlimited growth.139,141 The overwhelming majority of lesions present in children, with more than half presenting at birth and 90% discovered by the age of 2 years.136,137,144,145,146 Fewer than 10% are found in adults.141 Retroperitoneal cystic lymphangiomas are usually found in older children and adults. Acute symptoms result from infection, rupture, hemorrhage, or pressure on adjacent structures.137 Cystic lymphangiomas are usually isolated lesions, although posterior neck cystic lymphangiomas may be associated with Turner syndrome.147
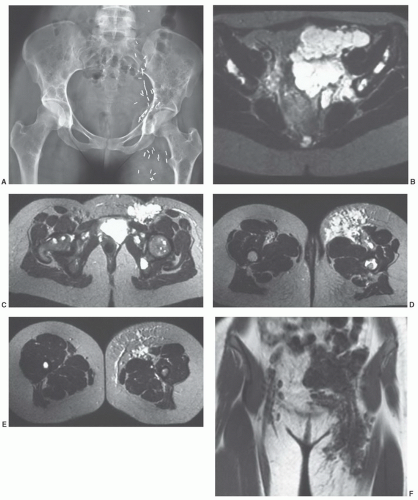 Figure 12.44 A 22-year-old woman with diffuse lymphangiomatosis involving bone and soft tissue. A: Anteroposterior radiograph of the pelvis demonstrating diffuse lucent areas in the femurs, pelvis, and sacrum. B-E: Axial T2-weighted images demonstrating diffuse pelvic and left thigh involvement. There are also bone changes in the iliac bones, both femoral heads, and the upper femur. Coronal (F) and sagittal (G) T1-weighted images demonstrating the anterior and posterior lymphangiomas. |
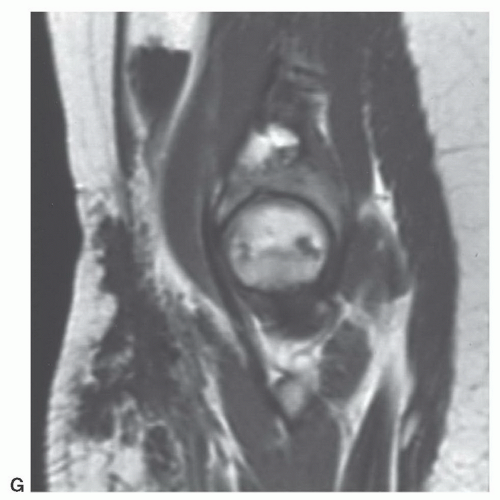 Figure 12.44 (continued) |
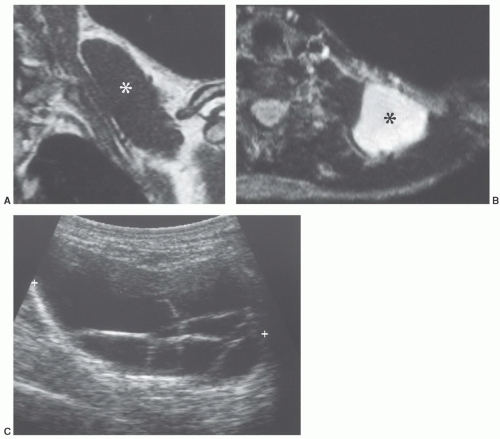 Figure 12.45 Lymphangioma in the neck of a 41-year-old woman. Coronal T1-weighted (A) and axial T2-weighted (B) images show the lesion (asterisk) to image similar to fluid. C: Ultrasound showed the lesion to be cystic with multiple septations. The MR appearance is nonspecific, and a myxoid tumor could have a similar appearance. The diagnosis was suggested preoperatively on the basis of both the MR and ultrasound appearances. |
Multiple lesions are unusual but have been reported.153 Local recurrence is not uncommon and may be seen in approximately 9% to 20% of cases.153,156 A malignant giant cell tumor of tendon sheath with metastases was reported by Carstens and Howell158; however, such lesions are quite rare.
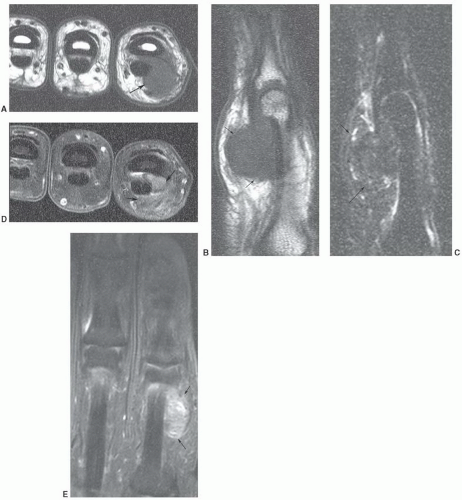 Figure 12.46 Giant cell tumor of tendon sheath. Axial (A) and sagittal (B) T1-weighted and sagittal fat-suppressed turbo spin-echo (C) images demonstrate the low signal intensity surrounding the flexor tendon (arrows). Post-contrast fat-suppressed T1-weighted images in the axial (D) and coronal (E) planes demonstrate inhomogeneous enhancement. |
of histiocytic-fibroblastic-myofibroblastic lesions.161,162 Maluf et al.161 noted that the lesions have an overlapping clinical presentation, with similar patient age and gender as well as lesion location and distribution. In addition, these lesions share similar growth patterns, showing a lobulated architecture. Although the microscopic appearance varies, both lesions contain spindle cells and multinucleated giant cells and share similar immunohistochemical attributes. Hence, the fibroma and giant cell tumor of tendon sheath may represent end points of a spectrum of cellular proliferation.162,163 It has been our experience that these lesions will show a similar appearance atMRI (Fig. 12.47).163
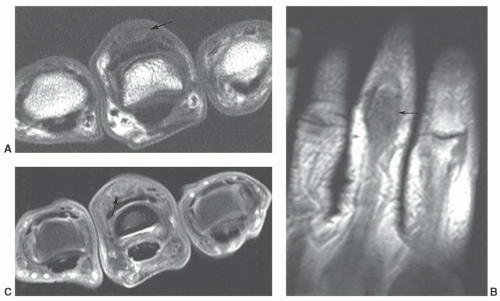 Figure 12.47 Fibroma of tendon sheath. Axial (A) and coronal (B) T1-weighted images demonstrate a well-defined low intensity lesion involving the extensor tendon (arrow). Post-contrast fat-suppressed T1-weighted axial image (C) demonstrates inhomogeneous enhancement (arrow). |
the knee (26%).164 Bone erosive changes are usually geographic lytic lesions with well-defined thinly sclerotic margins. They are most characteristic when they are multiple and are seen on both sides of the joint. The joint space is usually preserved, as is bone density.164 Uncommonly, radiographs will demonstrate an osteoarthritis appearance, with typical osteophytes, sclerosis, cysts, and joint narrowing, or an arthritis-like appearance, with concentric joint space loss, osteoporosis, and erosions.167 Radiologic calcification within the mass has been reported174 but is extremely
unusual and should suggest an alternative diagnosis. Calcification has also been reported in diffuse giant cell tumor of tendon sheath.175
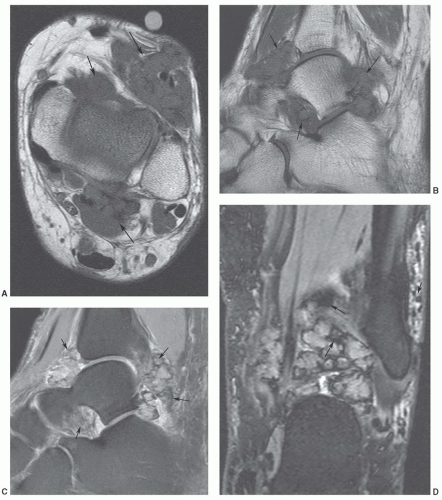 Figure 12.48 Pigmented villonodular synovitis in the ankle. Axial (A) and sagittal (B) T1-weighted images demonstrate a lobulated low signal intensity mass (arrows) about the ankle. Sagittal T2-weighted turbo spin-echo image shows areas of low signal intensity (arrows). Coronal DESS image (D) demonstrates multiple areas of blooming due to hemosiderin deposition (arrows). |
synovial inflammation and proliferation.152,169 The lytic bone lesions seen on radiographs and joint effusions are typically seen well on MRI.152 The diffuse giant cell tumor of tendon sheath has a skeletal distribution similar to that of PVNS and is often considered an extra-articular extension of PVNS. Its MRI signal intensity characteristics are similar to PVNS (Fig. 12.49).
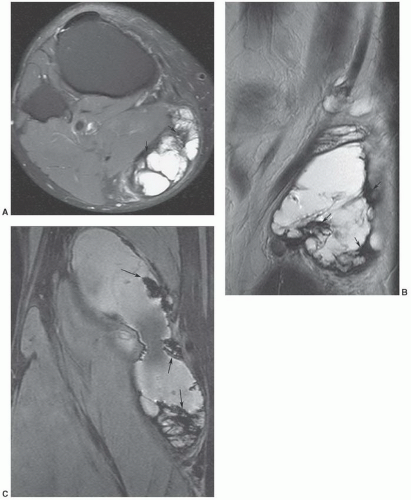 Figure 12.49 Diffuse giant cell tumor of tendon sheath. Axial (A) and sagittal (B) T2-weighted turbo spin-echo images demonstrate a large soft tissue mass below the knee with areas of low signal intensity (arrows). Coronal gradient-echo image (C) demonstrates blooming due to hemosiderin deposition (arrows). |
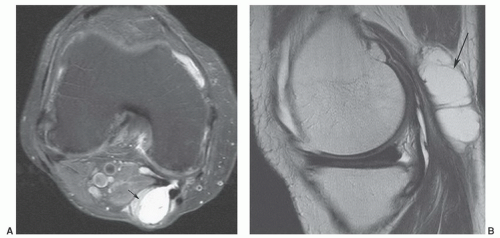 Figure 12.50 Popliteal cyst. Axial (A) and sagittal (B) fat-suppressed proton density-weighted images demonstrating fluid extending into the gastrocnemius semimembranosus bursa (arrow). |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


