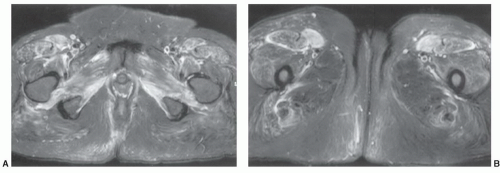
 Figure 15.1 Axial fat-suppressed fast spin-echo T2-weighted images at the level of the ischial tuberosities (A) and the proximal thighs (B) demonstrating an infiltrative process in the adductor muscles and anterior musculature, predominantly the tensor fasciae latae due to polymyositis. |
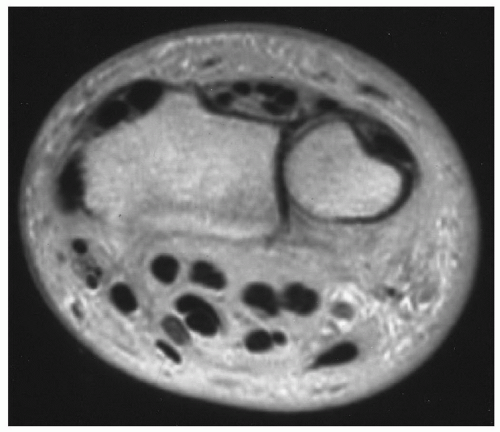 Figure 15.2 Axial proton density image of the wrist demonstrating complete fatty replacement of the muscles due to a chronic neuropathy. |
standardized documentation of disease activity and tissue damage.34
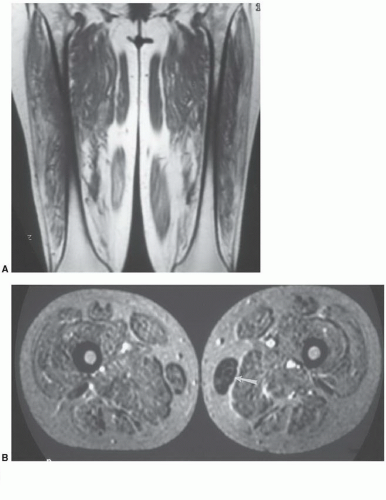 Figure 15.3 Duchenne muscular dystrophy. Coronal T1-weighted (A) and axial T2-weighted (B) images in a patient with Duchenne muscular dystrophy. All muscles are involved except for partial sparing of the gracilis (arrow) on the left. |
Table 15.1 MR Grading of Duchenne Muscular Dystrophy | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
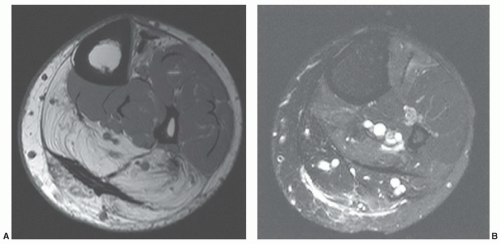 Figure 15.4 Neuropathic myopathy. Axial T1-weighted (A) and fast spin-echo T2-weighted images demonstrate increased signal intensity in the posterior compartments on the T2-weighted image (B) and fatty replacement on the T1-weighted image (A) due to tibial nerve compression. |
tenderness. Muscle weakness and atrophy is common with chronic myositis (type 3).52 Patients typically present with single or multiple palpable nodules. Nodules may be tender to palpation. The myopathic type is symmetrical and presents with progressive weakness and muscle atrophy.21,55
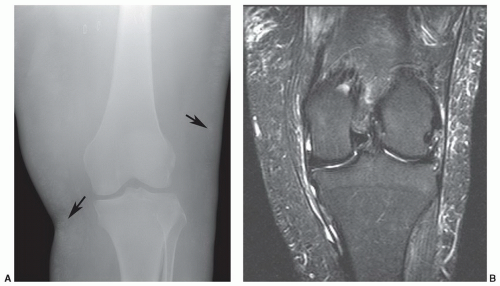 Figure 15.5 Dermatomyositis. A: AP radiograph of the knee demonstrating subtle subcutaneous soft tissue calcifications (arrows). Axial T1-weighted image (B) demonstrates low signal intensity in the subcutaneous fat (arrows) corresponding to the calcification on the radiographs. There is also significant muscle atrophy. Coronal STIR sequence (C) shows subcutaneous edema and edema along the ligaments and tendons. |
surrounding high signal intensity on T2-weighted or STIR sequences (Fig. 15.7). These findings are not specific and can also be seen with fibromatosis or other local inflammatory and neoplastic lesions.51,54 Myopathic changes (types 2 and 3) have nonspecific MR features with diffuse increased signal intensity on T2-weighted or STIR sequences. Biopsy is required to confirm the diagnosis.21,45,51,54
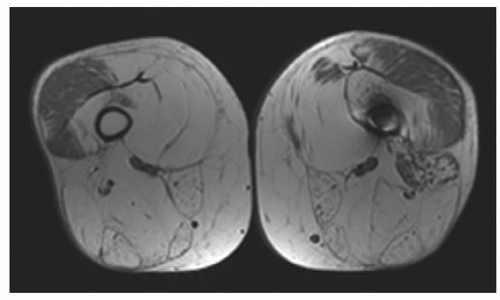 Figure 15.6 Polymyositis. Axial T1-weighted images demonstrating diffuse fatty infiltration and atrophy with relative sparing of the vastus lateralis. |
Table 15.2 Sarcoidosis Organ System Involvement | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||
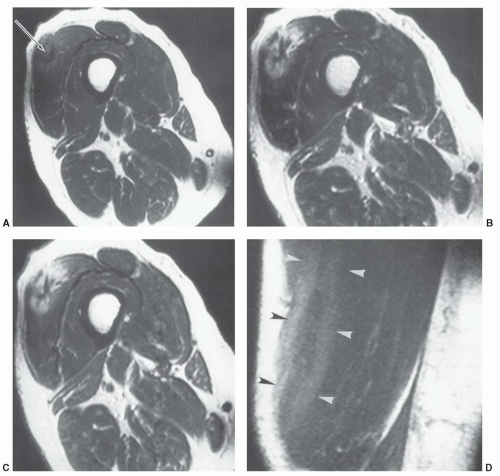 Figure 15.7 A 55-year-old woman with nodular sarcoid involving the vastus lateralis. A: SE 550/30 axial shows a stellate low intensity region (arrow) with slight increased intensity at the margin. SE 1,800/50 (B) and SE 1,800/100 (C) images show more obvious increased intensity surrounding the low intensity region. Coronal SE 550/30 image (D) shows three stripes (arrowheads) with outer increased and central decreased signal intensity. (From Otake S. Sarcoidosis involving skeletal muscle: imaging findings and relative value of imaging procedures. AJR Am J Roentgenol. 1994;162:369-375.) |
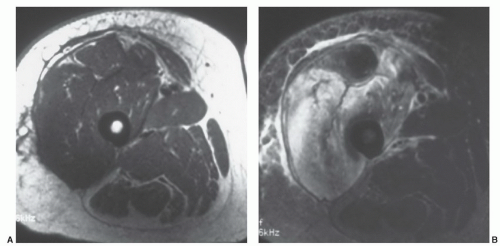 Figure 15.8 Diabetic muscle infarction. Axial T1-weighted (A) and T2-weighted (B) images of the thigh show fascial, subcutaneous, and vastus muscle inflammation. Changes are more easily appreciated on the T2-weighted image in B. |
or STIR sequences. Abnormal signal intensity in adjacent structure also occurs. The adjacent marrow may be involved in 32.5% cases, fascial planes in 35%, and adjacent joints in 26%.66 Fluid collections or abscesses are evident in 49% to 90% of cases. Yu et al.67 reported at least one abscess in 90% of patients (Fig. 15.10). Contrast-enhanced fat-suppressed T1-weighted images demonstrate peripheral enhancement of abscesses.61,64,66 Abscesses tend to be larger in patients with underlying diabetes.67 The majority of patients with abscesses are managed with surgical or image guided drainage procedures.66
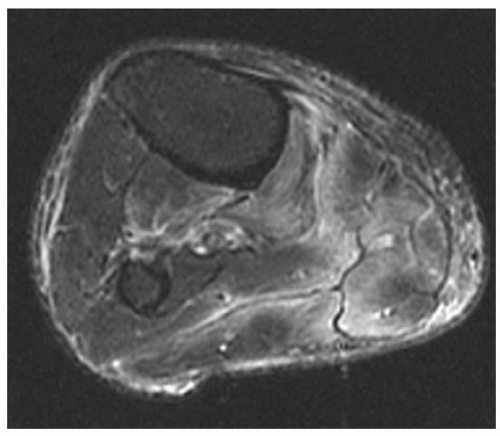 Figure 15.9 Ischemic myopathy in a diabetic. T2-weighted MR image demonstrating subcutaneous and subfascial increased signal intensity. |
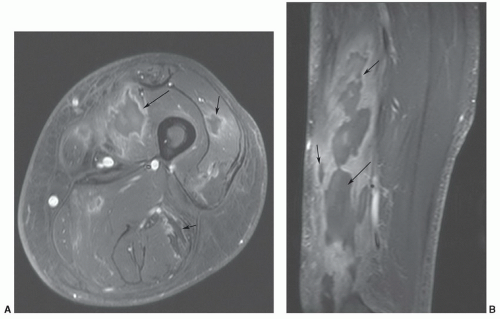 Figure 15.10 Bacterial pyomyositis. Post-contrast fat-suppressed T1-weighted axial (A) and sagittal (B) images demonstrating multiple abscesses with peripheral enhancement (arrows). |
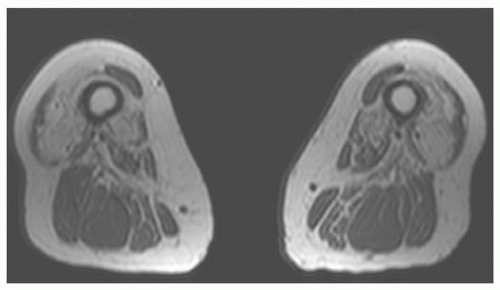 Figure 15.11 Inclusion body myositis. Axial T1-weighted images demonstrating marked atrophy and fatty replacement in the anterior compartment with partial sparing of the posterior compartment. |
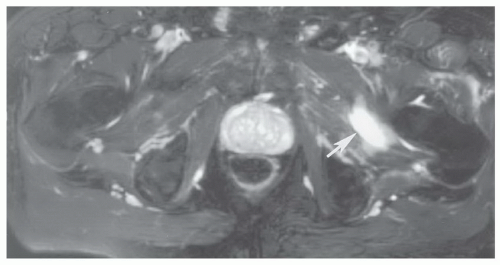 Figure 15.12 Adductor muscle tear. Axial fat-suppressed fast spin-echo T2-weighted image shows a grade 2 strain with increased signal intensity involving nearly 50% of the cross-sectional area and a focal hematoma (arrow). |
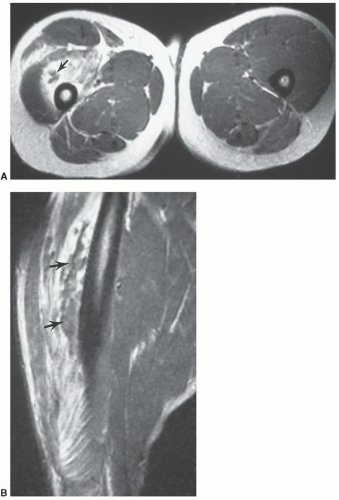 Figure 15.13 Grade 2 muscle strain with extensive edema and hemorrhage and low intensity hematoma (arrows) seen on axial (A) and sagittal (B) images. |
calcification is easily appreciated on CT studies. MRI demonstrates cystic changes on T1- and T2-weighted images. Calcifications may be more difficult to define if radiographs or CT are not available for comparison.80,81 Contrast enhancement does not facilitate the diagnosis (Fig. 15.17).65
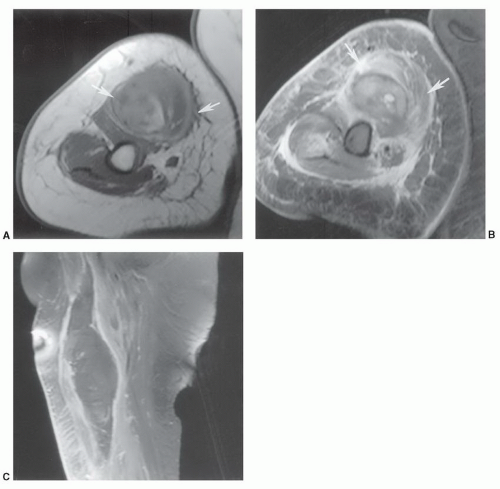 Figure 15.14 Grade 3 biceps tear with a large hematoma. Axial T1-weighted (A) and T2-weighted (B) images demonstrate a large hematoma (arrows) adjacent to the neurovascular structures. Sagittal contrast-enhanced T1-weighted image (C) shows the extent of the lesion with marginal enhancement. |
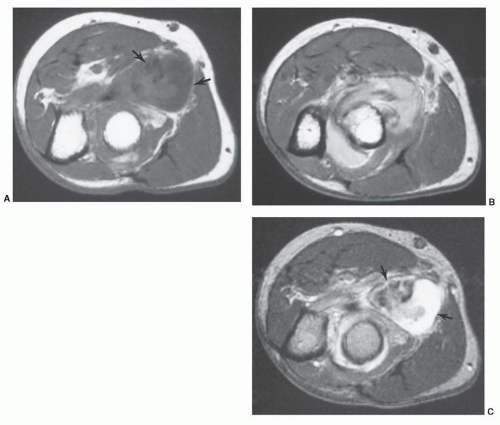 Figure 15.15 Hematoma in the proximal forearm related to biceps insertion tear. Axial T1-weighted (A), proton density (B), and T2-weighted (C) images show the inhomogeneous fluid collection (arrows). The hematoma compressed the radial nerve requiring surgical decompression. |
diagnosis of eosinophilic fasciitis. However, patients with active disease have characteristic MR features. These include fascial thickening, high signal intensity in the fascia on T2-weighted and STIR sequences, and enhancement following gadolinium administration (Fig. 15.19).88,89,90,91 These findings correlate with disease activity. Response to therapy and localization for biopsy are additional advantages of MRI imaging features. Currently, definitive diagnosis requires biopsy of cutaneous and muscle tissue.88,89,91
Table 15.3 Eosinophilic Fasciitis versus Scleroderma: Common Useful Distinguishing Features | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
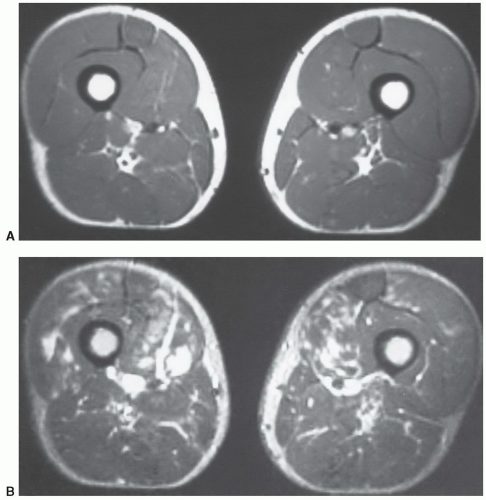 Figure 15.16 Bilateral rhabdomyolysis in an athlete. A: Axial T1-weighted image is normal. B: Axial T2-weighted image shows multiple areas of increased signal intensity in both thighs. |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


