infection.6,7,11 In children aged 1 or 2 years and up to 16 years of age, the growth plate prevents spread to the epiphysis. Therefore, joint space involvement is less common unless the metaphysis is intracapsular (Fig. 13.1).7,8,13,16
Table 13.1 Infections: Terminology and Categories | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
barefoot. Puncture wounds in the hand (i.e., thorns) occur when working with plants or gardening. Direct implantation may also occur when working in contaminated water or soil in the presence of skin abrasions.17,24,25,26
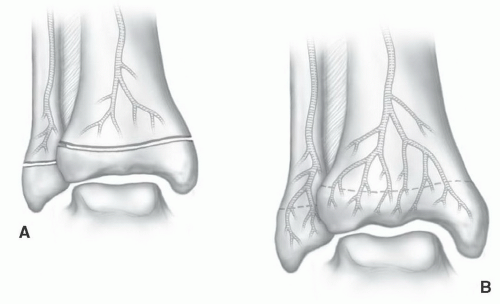 Figure 13.1 Illustrations of vascular patterns at the metaphyseal-epiphyseal junction in a child (A) and adult (B). The epiphysis is protected by the growth plate in patients 1 to 16 years of age. (From Berquist TH. Imaging of the Foot and Ankle. 3rd Ed. Philadelphia, Lippincott Williams & Wilkins, 2011.) |
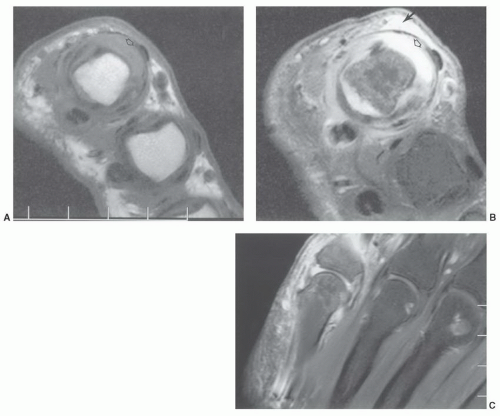 Figure 13.2 Fish hook injury with soft tissue infection extending into the fifth metacarpophalangeal joint. Axial T1- (A) and T2- (B) weighted images demonstrate soft tissue edema (arrow, B) and joint distention (open arrow). Fat-suppressed contrast-enhanced coronal T1-weighted image (C) shows enhancement of the soft tissues and synovial fluid. |
Table 13.2 Common Organisms in Musculoskeletal Infections | |||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 13.3 Atypical Mycobacterial Infections | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
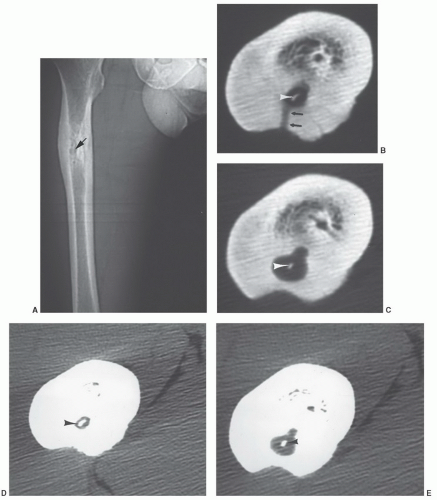 Figure 13.3 Chronic osteomyelitis with sequestrum and cloaca. A: CT scout images show medullary sclerosis and cortical thickening in the femur with a central lucency (arrow). Axial CT images with bone (B, C) and soft tissue (D, E) settings show a local abscess with a sequestrum (arrowheads in C and D) and cloaca (arrows). Beam hardening artifact degrades the image quality of the adjacent soft tissues. |
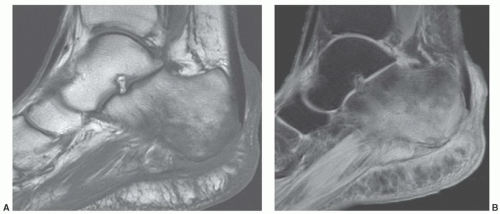 Figure 13.4 Sagittal T1- (A) and fat suppressed turbo spin-echo T2-weighted (B) images of the calcaneus demonstrating low signal intensity on T1- (A) and high signal intensity on the T2-weighted (B) images due to osteomyelitis in a diabetic. Routine radiographs were normal. |
We routinely add gadolinium-enhanced fat-suppressed T1-weighted images in patients with suspected osteomyelitis (0.1 mmol/kg b.w. intravenously) (Fig. 13.6).
 Figure 13.5 Osteomyelitis in the left femur. Coronal STIR sequence shows subtle thickening of the cortex with increased signal intensity in the marrow and adjacent soft tissues. |
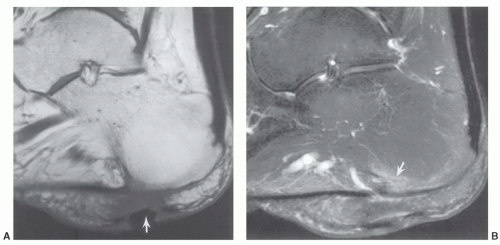 Figure 13.6 Diabetic with calcaneal osteomyelitis. A: Sagittal T1-weighted image demonstrates a soft tissue ulcer (arrow) and swelling. B: Contrast-enhanced fat-suppressed T1-weighted image demonstrates an area of enhancement (arrow) due to early osteomyelitis. |
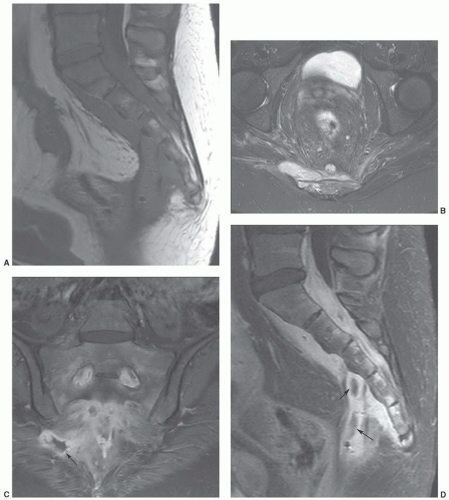 Figure 13.7 Patient with Crohn’s disease and sacral osteomyelitis with associated abscess formation. Sagittal T1- (A) and axial T2-weighted (B) images demonstrate perisacral soft tissue inflammation with an anterior soft tissue mass on the T1-weighted image and an area of soft tissue mass lateral to the sacrum on the T2-weighted image. Coronal (C) and sagittal (D) post-contrast fat suppressed T1-weighted images demonstrate the peripherally enhancing abscesses (arrows). |
for CT. Both techniques were equally specific for excluding osteomyelitis. Gallium-67 and indium-111 labeled white blood cells are more specific for infection than technetium scans.28,56 Beltran et al.57 compared technetium-99m methylene diphosphonate (MDP), gallium-67, and MRI for evaluating musculoskeletal infection. All techniques were equally effective in detecting osseous infection. However, MRI was more sensitive (100% compared to 69% for isotope scans) in identifying abscesses and distinguishing abscesses fromcellulitis (Fig. 13.7).57 Contrast enhancement and diffusion-weighted imaging add to the ease of detection of abscesses.4,31,55,59
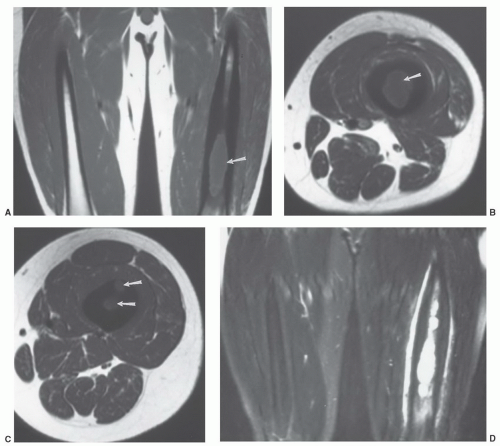 Figure 13.8 Osteomyelitis in the femur. Coronal (A) and axial (B and C) T1-weighted images demonstrate loss of normal fatty marrow in the femur (arrows). Signal intensity is increased on T2-weighted coronal image (D). Post-contrast fat suppressed T1-weighted images (E-H) demonstrate areas of peripheral enhancement in bone due to abscess formation. Juxtacortical soft tissue enhancement is also seen. |
agree that sensitivity for detection of infection is improved by contrast-enhanced imaging. However, findings are not specific in differentiating infection from inflammation or neoplasms.47 Lack of bone enhancement effectively excludes infection.47,53,59
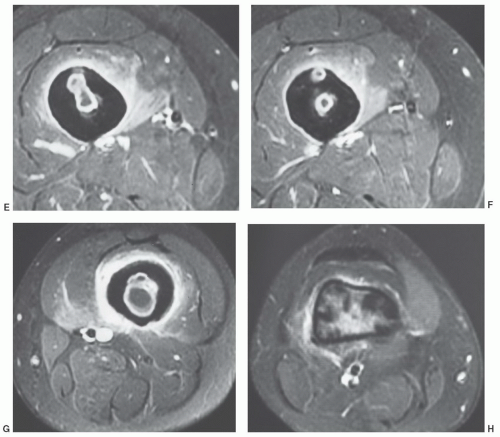 Figure 13.8 (continued) |
Spinal involvement (accounts for 50%) of musculoskeletal involvement and tuberculous arthritis (accounts for 60%) respectively remain the most common sites of involvement (Fig. 13.10).64,70 Extraspinal osteomyelitis accounts for 19% of musculoskeletal tuberculosis. Pulmonary tuberculosis is evident in about 50% of patients with musculoskeletal involvement.70 Tuberculous osteomyelitis involves the metaphysis or epiphysis similar to pyogenic osteomyelitis. Periosteal reaction, bone sclerosis, and sequestra are less common than pyogenic infection.61,70 Changes may
resemble a benign bone tumor or, if more aggressive, round cell lesions such as Ewing sarcoma, lymphoma, or leukemia.7,31 CT, radionuclide scans, and MRI frequently add little to the specificity of the pathology.61,69 Therefore, biopsy and culture are required.
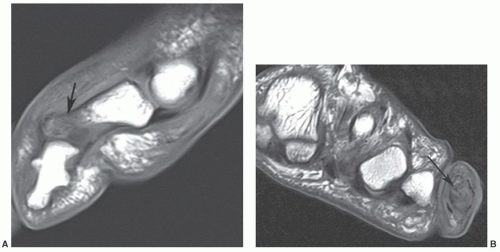 Figure 13.9 Sagittal (A) and axial (B) T1-weighted images of the fifth toe demonstrating decreased signal intensity in the distal aspect of the phalanx (arrow) in a confluent pattern due to osteomyelitis. The distal phalanges are congenitally fused. (From Berquist TH. Imaging of the Foot and Ankle. 3rd Ed. Philadelphia, Lippincott Williams & Wilkins, 2011.) |
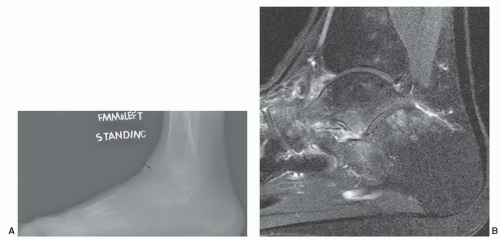 Figure 13.10 Multifocal tuberculosis. A: Lateral radiograph of the foot and ankle demonstrates marked osteopenia in the ankle, mid and hind foot. There is also an ankle effusion (arrow). Sagittal T2-weighted image (B) demonstrates periarticular marrow edema and axial (C) and sagittal (D) post-contrast fat-suppressed T1-weighted images demonstrate extensive bone and soft tissue involvement with synovial enhancement (arrow). Sagittal T1- (E) and T2-weighted (F) images of the spine demonstrate disc and osseous involvement at T12-L1 (arrow). (From Berquist TH. Imaging of the Foot and Ankle. 3rd Ed. Philadelphia, Lippincott Williams & Wilkins, 2011.) |
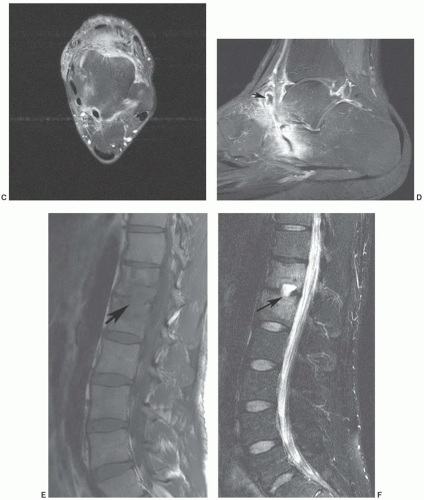 Figure 13.10 (continued) |
caseating necrosis in tubercular granulomas. The second image feature described was low intensity with marginally higher intensity peripherally on T1-weighted images. Surrounding edema was common in this setting. Extraosseous soft tissue edema and abscess formulation were evident in about 80% of cases.61
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


