Fig. 1
Mini-open incision. The circle is marked around the anterior superior iliac spine (ASIS) and the surgical incision starts 1 cm lateral and 1 cm inferior to the ASIS
Using a 10 blade scalpel, the incision should be extended through the subcutaneous tissue and bleeding should be controlled by electrocautery. The teeth of a Hibbs retractor can be used on the medial side for retraction, and should be held by one assistant. For deeper subcutaneous tissue, a second Hibbs retractor can be used on the lateral side and should be held by a second assistant. Careful dissection using a scalpel should be performed to avoid damage to the lateral femoral cutaneous nerve and until the tensor fascia lata (TFL) is identified (Fig. 2).
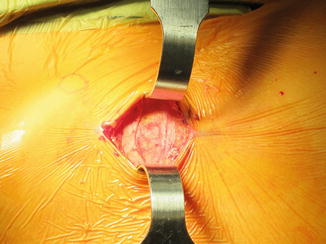
Fig. 2
The fascia of the tensor fascia lata is the first layer of the approach
The TFL is then cut longitudinally inline with the fibers (Fig. 3) and the index finger is used to sweep underneath the fascia. The Hibbs retractors should be reversed and the hook end should be used to retract the fascia on either side. The interval between the TFL and sartorius should be identified by finding two distinct muscle bellies (Fig. 4). Finger dissection should be performed through this interval and the TFL muscle should be swept laterally and the sartorius should be swept medially. The Hibbs retractors should be replaced deeper with the hook ends to retract the TFL and sartorius.
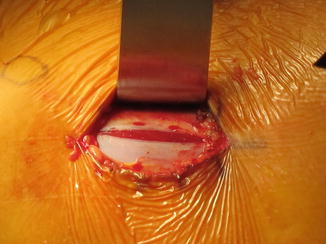

Fig. 3
A vertical incision is carried through the TFL using a 10 blade scalpel
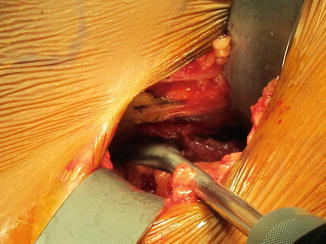
Fig. 4
The second layer of the approach is the first internervous interval between the sartorius and TFL
Since this is the mini-open approach, the ascending branches of the lateral femoral circumflex artery and vein may not be exposed in the distal region of the incision between the TFL and sartorius. If the blood vessels are not visualized, they do not need to be cauterized. If they are exposed, then the ascending branches of the lateral femoral circumflex vessels should be cauterized prior to proceeding, to prevent bleeding that may compromise visualization of the surgical field.
Dissection through the TFL and sartorius are carried out until the silver muscle belly of the rectus femoris can be identified (Fig. 5). The plane between the gluteus medius and rectus femoris can be identified.

Fig. 5
The silver muscle belly of the rectus femoris denotes the second internervous interval before the hip capsule
Care should be taken to preserve the straight head of the rectus femoris that is attached to the anterior inferior iliac spine (AIIS) and the reflected head that is attached to the superior acetabular brim. Occasionally, there are tight bands of the rectus femoris superiorly that can be released using electrocautery without releasing the entire origin of the muscle. Once the plane between the rectus femoris and gluteus medius is developed, the hip capsule should be visible. To provide adequate visualization of the hip capsule, one long handled narrow blunt Hohmann retractor should be placed around the calcar and another long handled narrow blunt Hohmann retractor should be placed around the greater trochanter. To gain visualization superiorly, a Cobb elevator should be used to develop the plane above the AIIS for placement of a lighted superior retractor with a tooth (Fig. 6).
 Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum




Related posts:
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Femoral Head Fractures
Surgical Technique: Osteochondral Autograft Transfer and Osteochondral Allograft Transplant for Preservation of the Femoral Head and Acetabulum
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
