21 Meniscal Injuries/Repair: T-Fix
The surgical effort to salvage a meniscus tear by repair recognizes the importance of this structure. The meniscus provides stability and is important in load transmission, joint lubrication, and articular cartilage nutrition. Degenerative changes are well documented after total or subtotal meniscal removal. There are several repair approaches, including the inside-out, outside-in, and allinside techniques. The T-fix offers a clinically successful all-inside approach that uses sutures anchored in the outside capsule area.1–3
Indications
- Longitudinal, peripheral meniscal tears with a good blood supply. Typically this is a tear either at the synovial meniscal junction or in the red/white region.
- Tear length: longer tear lengths do not heal as well. Tears between 1.5 and 2 cm have better success.
- Tears in the posterior medial or posterior lateral corner where other techniques might injure neurovascular structures
Contraindications
- Good meniscal blood supply is crucial; therefore, avoid repairs in older patients and horizontal cleavage tears.
- Degenerative articular cartilage change
- Allergy to plastic
Physical Examination
- Joint line tenderness
- McMurray’s test (or other meniscal tests) positive
- Effusion
Diagnostic Tests
- Physical examination
- Knee radiographs
- Magnetic resonance imaging (MRI) (sometimes indicated)
Special Considerations
The outside-in single vertical suture is the “gold standard” for meniscal repair. Other techniques are designed to approach the good results of this technique. Most repairable meniscal tears are found associated with anterior cruciate ligament (ACL) injury. The surgeon performing an ACL reconstruction should be prepared to repair the meniscus at the same time. Healing rates for “isolated” meniscal repairs in stable knees are approximately 80%, whereas in knees undergoing ACL reconstruction it is 90 to 95%. The T-fix has a polyacetyl crossbar that is left permanently in place.
Preoperative Planning and Timing of Surgery
- Early intervention has not been demonstrated to improve the results. With the ACL-injured knee, it is desirable to wait until the effusion is resolved and good motion is established. This is even more critical when a meniscus repair is performed because of the tendency for postoperative stiffness.
- The T-fix technique requires mastery of arthroscopic knot tying using the appropriate knot pusher. Practice is required before this technique can be performed clinically.4
Special Instruments
- T-fix sutures attached to either curved or straight needles (single or double sutures)
- Probe to measure depth of meniscus
- T-fix knot pusher
Anesthesia
Options are general anesthesia, regional anesthesia, or local anesthesia.
Patient and Equipment Positions
- Patient is supine with knee in leg holder
- Standard knee arthroscopy setup
- Standard anterolateral, anteromedial, or central arthroscopy portals
- View through the ipsilateral (or central) portal and instrument through the contralateral portal
- To access the posterior medial meniscus, hold the knee slightly flexed with valgus stress. Access the posterior lateral meniscus by holding the knee in a figure-four position (~90 degrees) with varus stress.
- Arthroscopic cannulas are required for instrument insertion.
- Procedures to promote meniscal healing (vascular access channel punch, meniscal rasp, synovial abrasion) should be used.
Surgical Procedure
- Establish standard viewing portals. View through the ipsilateral (or central) portal and instrument through the contralateral portal.
- Encourage a healing response by rasping, creating vascular access channels, and synovial abrasion.
- Determine proper crossbar meniscal penetration depth using calibrated depth probe (4 or 5 mm is added to the measured depth to ensure proper seating) (Fig. 21–1).
- Cut the calibrated protective sleeve to this length.
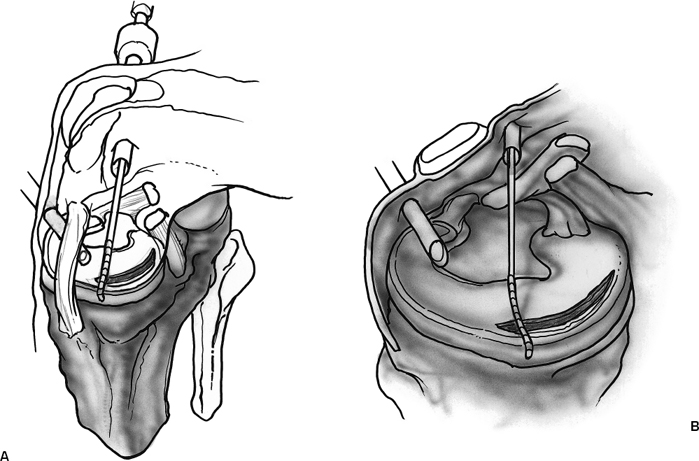
- Insert the spinal needle into the meniscus until this protective sleeve hits the meniscal surface. A gentle give is felt when the needle passes through the posterior meniscus (Fig. 21–2).
- Place the push rod (obturator) into the spinal needle and deploy the T-fix (Fig. 21–3).
- The insertion needle is removed and the toggle anchor seated by traction on the suture (Fig. 21–4).
- Additional sutures are placed at 4- to 5-mm intervals (Fig. 21–5).
- A knot (using a series a half hitches) is tied with the knot pusher and the sutures cut (Fig. 21–6).
- Place sutures every 4 to 5 mm until repair is completed (Fig. 21–7).
- Cut the calibrated protective sleeve to this length.
Dressings, Braces, Splints, and Casts
- A simple absorptive sterile dressing is applied to the skin.
- Compression with Ace bandage
- Progressive weight bearing with crutches as needed
Tips and Pearls
- Practice knot tying several times before this technique is attempted.
- The T-fix must be placed through a working cannula.
- The polyacetyl bar may not actually exit the capsule, but if it toggles enough a secure suture is the result.
- If placing two knots, the central anchor should be double stranded.
- The T-fix devices can be placed to allow a vertical orientation of the suture.
Pitfalls and Complications
- This technique is technically challenging. It requires arthroscopic knot tying using a nonslip knot made up of four half-hitches.
- Horizontal suture placement has been shown to produce lower pullout strengths than vertical orientation.5
- The polyacetyl (plastic) foreign body is permanent.
- The knot on the meniscal surface becomes more prominent as more half-hitches are placed, and four half-hitches do not mean these are square knots.
Postoperative Care and Rehabilitation
- For meniscal repairs performed in association with ACL reconstruction, the usual ACL reconstruction protocol should be followed.6
- Loaded knee flexion should not exceed 90 degrees for the first 8 weeks.
- Early motion is permitted as swelling decreases.
- Weight bearing as tolerated is permitted.
- When there is no effusion, full extension, and flexion to 135 degrees, straight-ahead jogging is permitted.
- Full pivoting sports may begin when there is no pain, swelling, or reduced motion despite running and agility training.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


