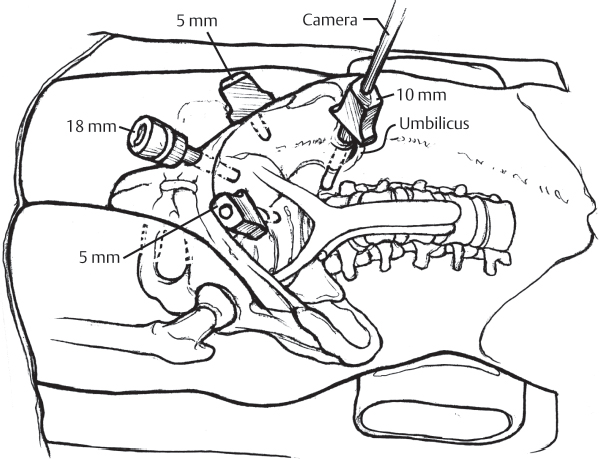
58 Anterior lumbar interbody fusion (ALIF) has traditionally been a technique widely utilized by spine surgeons for the treatment of many disorders. Given the ability to visualize the anterior lumbar spine directly, ALIF has been used to treat spondylolisthesis, degenerative disk disease (DDD), spinal deformities, spinal infections, trauma, and tumors. When used to treat DDD, ALIF may be performed as a stand-alone procedure or in combination with a posterior surgery. Traditionally, open retroperitoneal approaches have been the mainstay of treatment. Limited-access approaches have been developed over the years, including laparoscopic techniques. Over the past decade, laparoscopic approaches for DDD have lost popularity to other techniques that may accomplish similar goals. With the increased use of transforaminal lumbar interbody fusion (TLIF) and a variety of direct lateral techniques, laparoscopic techniques are not commonly used today for the treatment of DDD. There are no current classifications that direct toward a specific ALIF or interbody technique for DDD. Generally, ALIF may be performed as a stand-alone procedure or in combination with posterior fusion and instrumentation. ALIF can be performed through an open, mini-open, or laparoscopic approach. ALIF, regardless of the technique, should be considered for DDD only when the patient has been carefully selected. Surgical candidates for lumbar fusion should have an anatomically identifiable pain generator that corresponds to their symptoms and have failed at least 6 months of extensive nonoperative treatment for their condition. As it pertains to laparoscopy, the patient’s previous peritoneal or retroperitoneal surgical history is of utmost importance when considering an anterior approach. Laparoscopic approach or not, the patient’s physical examination should be consistent with the location and nature of symptoms. There are many non-specific sources of back pain that are not amenable to spinal surgery and that should be kept closely in mind. DDD may cause primarily axial lumbar pain but may also be associated with nerve root compression; a detailed neurologic examination is critical. When treating DDD surgically, all imaging studies should point to the same level or levels as the source of the pain. Imaging studies such as plain radiographs, magnetic resonance imaging (MRI) and computed tomography (CT) scans are often utilized. Lumbar diskography has been a controversial test that has been traditionally used as a confirmatory test as to the pain generator. With some studies suggesting the potential for accelerated deterioration of lumbar disks and the potential decreased usefulness of this test, diskography should be used sparingly and after patient counseling. Exhausting nonoperative treatment is imperative when considering surgical candidates for DDD. Extensive physical therapy, activity modification, weight control, smoking cessation, nonsteroidal anti-inflammatory drugs (NSAIDs) and possible interventional pain management modalities should all be considered. Patient selection has a significant effect on outcomes, often regardless of specific technique used. Laparoscopic ALIF is performed with the patient supine on a radiolucent operating table to allow fluoroscopic visualization of the spine during the procedure. An endoscopic transperitoneal approach uses several portals for the endoscope and insufflators, and two or more working portals to allow for dissection, retraction, and discectomy (Fig. 58.1). Lumbar laparoscopy requires an absolute understanding of the vascular anatomy around the disk. A cross-sectional review of the MRI and/or CT should be done preoperatively to make sure there are normal anatomic landmarks. A high-riding L5–S1 level may behave like an L4–L5 level in terms of dissection and make the approach more challenging. Approaching L4–L5 laparoscopically is challenging and should generally be performed only by experienced laparoscopic spinal surgeons. Vascular dissection at L4–L5 with mobilization of the common iliac vein and the iliolumbar branch requires extensive experience using the laparoscopic techniques (Fig. 58.2). Fig. 58.1 An endoscopic transperitoneal approach is demonstrated using a portal for the endoscope, one for the insufflators, and two working portals to allow for dissection, retraction, and discectomy.
Lumbar Laparoscopy
![]() Classification
Classification
![]() Workup
Workup
History
Physical Examination
Imaging Studies
![]() Treatment
Treatment
Nonoperative Treatment
Surgical Technique
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


