Ligament Advancement in Total Knee Arthroplasty
Patient Presentation and Symptoms
- Knee degenerative arthritis
- Severe valgus deformity and medial thrust
- Severe varus deformity and lateral thrust
Indications
- Severe valgus deformity with elongation of the medial supporting structures
- Severe varus deformity with elongation of the lateral supporting structures
- Soft tissue release to correct deformity will cause undesirable leg lengthening.
- Well-fixed components with collateral instability
- Failed constrained implant due to soft tissue imbalance
Contraindications
- Inadequate supporting ligaments
- Inadequate bone stock
Physical Examination
- Alignment
- Range of motion
- Collateral stability
- Muscle strength
- Neurovascular status
- Gait
Diagnostic Tests
- Radiographs: anteroposterior (AP), lateral, and Merchant skyline view
- Long-standing radiograph that includes the hip, knee, and ankle
Special Instruments
- Drill
- Screws and washers
- Bone staples
- No. 5 nonabsorbable suture material
Anesthesia
Epidural with intravenous sedation, or general anesthesia
Patient Position
Supine with the involved leg draped free
Surgical Procedure
Surgical Approach
- Standard midline skin incision
- Medial parapatellar arthrotomy
Medial Ligament Advancement
- Exposure of the medial epicondyle
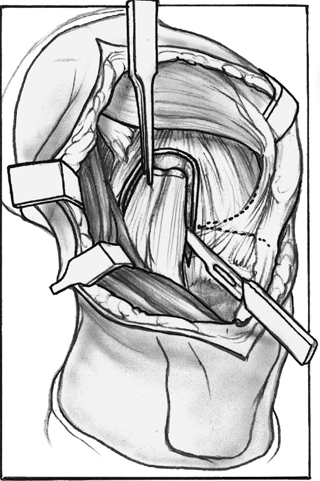
- Incise around the medial supporting structures including the deep and superficial medial collateral ligament and the posterior oblique ligament.
- The flap is released proximally and elevated subperiosteally in a distal direction.
- The flap created is trapezoidal in shape. The superficial medial collateral ligament is anterior and the posterior oblique ligament is posterior (Fig. 45–1).
- The medial ligament advancement is performed after fixation of the final components.1,2
- With No. 5 nonabsorbable suture material, two locking stitches are placed in the medial flap (Fig. 45–2).
- Soft tissue proximal to the medial epicondyle is elevated to allow the advanced tissue to sit on bare bone.
- The medial flap is advanced proximally and anteriorly.
- The sutures are tied around a screw and washer. 10. A staple is placed at the medial epicondyle to fix the ligament at the center of rotation (Fig. 45–3).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


