Humeral diaphyseal fractures
INTRODUCTION
The incidence of diaphyseal humerus fractures nearly doubles with every decade of life after age 60.1 The management of diaphyseal humerus fractures in elderly patients merits specific considerations. On the one hand, elderly patients may be less able to adapt to restricted use of the affected extremity during non-operative treatment. They may not be able to live independently. On the other hand, operative fixation must account for challenges in achieving adequate fixation in osteoporotic bone and the potential for increased medical risks.
ANATOMY
The AO classification system defines the proximal and the distal segments of long bones by a square whose sides have the same length as the widest part of the epiphysis; the diaphysis is the remaining middle portion of the bone (Figure 22.1). The humeral diaphysis is covered by muscle on all sides, contributing to a good blood supply and high union rates. The extensive range of motion at the shoulder helps patients compensate for relatively substantial angular deformity of the humeral shaft.
EPIDEMIOLOGY
The majority of diaphyseal humerus fractures occur in elderly patients after a simple fall.1 The annual incidence of diaphyseal humerus fractures among the elderly in the United States was estimated as 12.0 or 23.5 per 100,000.2,3 In a study of 361 humeral shaft fractures in Europe, Ekholm et al. reported a bimodal age distribution with a minor peak in the third decade represented by young men sustaining high-energy trauma, and a second major peak in the eighth decade attributed to low-energy falls in elderly women (Figure 22.2).1 Whereas most fractures occurring in patients up to age 50 are attributed to high-energy mechanisms, among patients older than 50 years, over 75% occurred in women and were due to a fall from standing height.4
EVALUATION AND CLASSIFICATION
A fracture caused by relatively minimal trauma should raise suspicion for pathological fracture through a tumour. Loss of consciousness may point to syncope or an underlying cardiac condition.
The reported mechanism should be consistent with the fracture pattern. For example, a spiral fracture is typically caused by a rotational force rather than by a direct lateral blow. Discordance between the history and objective findings is a hallmark of domestic or elder abuse.5,6 The PRAISE study recently revealed that 1 in 6 women presenting to an orthopaedic clinic has a history of abuse within the past year, and 1 in 50 women present as a direct consequence of intimate partner violence.6 Although no specific fracture pattern is considered pathognomonic of elder abuse, suspicion may be raised by implausible or vague explanations provided by the patient or caregiver, delays in seeking medical treatment, frequent emergency room visits and partially healed fractures.5
When associated with high-energy polytrauma, Advanced Trauma Life Support (ATLS) guidelines should be followed to resuscitate and stabilize a trauma patient prior to addressing the humerus fracture. In the setting of a high-energy injury, humeral shaft fractures may be associated with intra-abdominal injuries.7
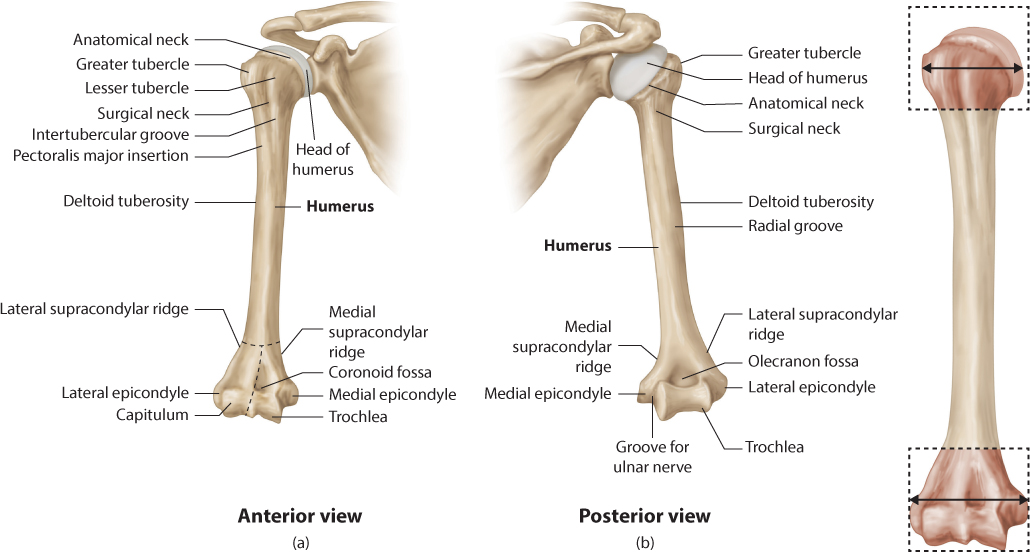
Figure 22.1 (a) Anatomy of the humerus. (b) AO definition of the humeral diaphysis. The proximal and the distal segments of long bones are defined by a square whose sides have the same length as the widest part of the epiphysis (Adapted from Netter images, Image ID 9183, available at https://www.netterimages.com/osteology-anterior-and-posterior-view-of-the-humerus-labeled-thompson-2e-orthopaedics-frank-h-netter-9183.html).
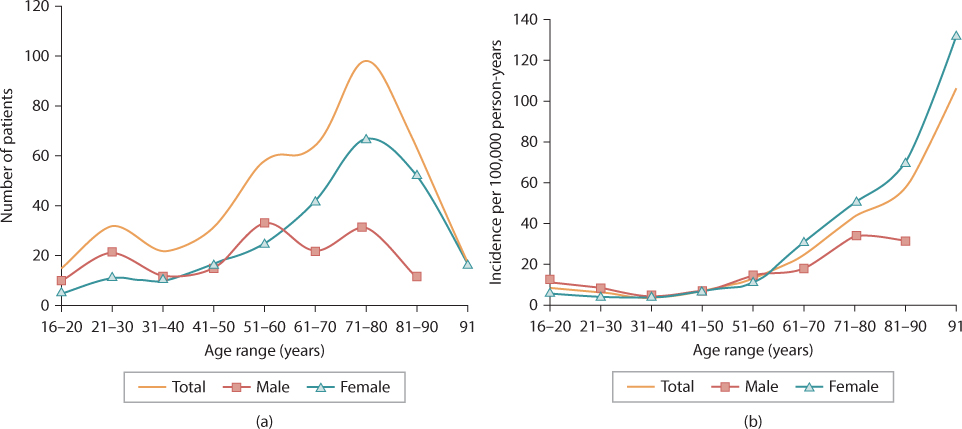
Figure 22.2 (a) Age distribution of 401 humeral diaphyseal fractures and (b) age- and gender-specific incidence of humeral diaphyseal fractures as reported by Ekholm et al.1
The upper extremity is evaluated for swelling, ecchymosis, deformity, open wounds, and neurologic or vascular deficits, with particular attention to the radial nerve. Extensive ecchymosis is common, and typically tracks down the arm as blood pools distally. The classic varus deformity arises due to abduction of the proximal fragment by the deltoid, and adduction and proximal migration of the distal humerus by the biceps and triceps.
Neurovascular injuries should be documented prior to treatment; Sarmiento et al. reported an 11% incidence of radial nerve palsies.8 The motor component of the radial nerve is best assessed by testing the extensor carpi radialis longus (ECRL) or extensor digitorum communis (EDC). The ECRL can be examined by positioning the patient in approximately 90 degrees of elbow flexion and testing resisted wrist dorsiflexion. Note that interphalangeal joint extension is facilitated by the lumbricals, which are innervated by the ulnar nerve, and therefore does not assess isolated radial nerve function. To examine EDC function, have the patient extend the metacarpophalangeal joints with the proximal interphalangeal joints flexed. All of these tests may be affected by guarding associated with pain from the fracture. The surgeon may need to coach and reassure the patient to get a good examination of motor function.
Although open humeral shaft fractures are uncommon (2–10%),1,4 any superficial wounds must raise suspicion for open fracture and should accelerate the evaluation and treatment process (Figure 22.3). Due to the relatively loose investing fascia and the large potential spaces within the anterior and posterior compartments of the arm, compartment syndrome is rare, especially after low-energy falls in the elderly.
Imaging
The entire humerus, elbow and shoulder should be visualized on radiographs in at least two planes to evaluate alignment and rotation. In patients who are unable to abduct the arm for a lateral view of the humerus, a transthoracic lateral radiograph may be obtained with the patient standing and the contralateral arm raised above the head to avoid superimposition of both arms (Figure 22.3c). On occasion, computed tomography (CT) can help evaluate rotational deformity, intra-articular extension or potential arterial injury using CT angiography.
Pseudosubluxation refers to the transient inferior subluxation of the humeral head relative to the glenoid, often associated with humerus fractures.9 This phenomenon occurs due to deltoid and rotator cuff atony, usually as a result of inhibition of the deltoid due to pain, but sometimes related to concomitant axillary nerve palsy. In the setting of a humerus fracture, pseudosubluxation is usually a transient and benign finding that resolves with time and does not require extensive testing, reduction maneuvers or surgical intervention. Active isometric firing of the deltoid, biceps and triceps, combined with sling support when not exercising, restores the anatomic shoulder joint alignment by approximately 6 weeks in 92% of patients.9
Classification
Humeral shaft fractures are commonly classified by location (proximal, middle or distal third) and pattern (transverse, butterfly, comminuted, spiral, oblique). The relatively low incidence of open humeral shaft fractures can be attributed to the low-energy mechanism of injury of most humeral shaft fractures, as well as the extensive muscle coverage throughout the humeral shaft. Wounds can be classified by the Gustilo–Anderson classification.10
Goals of treatment
The primary goal of treatment for a humeral shaft fracture is healing with good shoulder and elbow motion. Given the global mobility of the shoulder, deformity has a limited influence on function, and up to 30 degrees of angulation is accepted.
NON-OPERATIVE TREATMENT
Initial splinting
Non-operative treatment of humeral shaft fractures consists of three phases: initial splinting, functional bracing or casting, and rehabilitation.11
Initially, the arm is typically immobilized in 90 degrees of elbow flexion with a coaptation splint that extends from the medial aspect of the axilla, around the elbow, over the lateral aspect of the shoulder and to the neck (Figure 22.4a). The purpose of coaptation splinting is to stabilize the fracture and thereby improve patient comfort. Coaptation splinting employs dependency traction and hydrostatic pressure to maintain fracture reduction and is indicated for fractures with minimal shortening, and for short oblique or transverse fracture patterns. Coaptation splints are cumbersome for patients and can be associated with pressure ulcers, therefore they should be used only in the initial treatment, as a bridge to either a functional brace or a hanging cast.
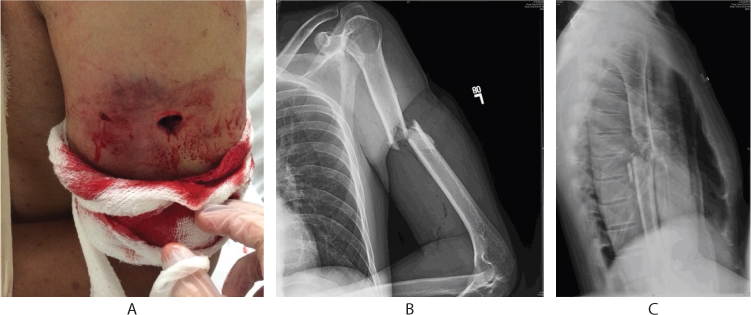
Figure 22.3 Open mid-diaphysis humerus fracture. (a) Open wound on lateral aspect of the arm. (b) Anteroposterior and (c) transthoracic lateral radiographs.

Figure 22.4 Non-operative treatment modalities for humeral diaphysis fractures. (a) Coaptation splint. (b) Functional (Sarmiento) brace. Note the forearm and hand swelling that may occur with prolonged bracing. (c) Hanging arm cast.
Hanging casts were first described by Caldwell in 1933.12 A cast is applied extending from the proximal humerus to the wrist, with the elbow flexed at 90 degrees and the wrist in neutral position; a sling is passed around the neck and through a loop on the distal aspect of the cast for support (Figure 22.4c). Hanging casts effect and maintain fracture reduction through gravity traction, with the arm hanging freely when the patient is awake. They offer better control of varus angulation in distal third fractures. This approach is a definitive mode of treatment that can be applied immediately, but may be cumbersome for the elderly. Many avoid hanging casts due to concerns about elbow stiffness, although recent data suggest no difference in elbow motion between patients who use casts and those who use functional braces (Jawa A. Personal communication. From Ring D, Boston, MA, 2015).
Functional bracing
Functional bracing was introduced by Sarmiento et al. in 197713 and remains the mainstay of non-operative treatment for humeral shaft fractures. The term ‘functional bracing’ refers to a prefabricated brace that is applied circumferentially around the arm and thereby permits motion of the shoulder and elbow (Figure 22.4b). In theory, a functional brace employs three principles intended to maintain fracture reduction. First, active muscle contraction corrects rotation and angulation. Second, soft tissue compression exerts a ‘hydraulic effect’, which assists in aligning fracture fragments. Finally, and perhaps most importantly, gravity assists with alignment. The brace consists of two plastic sleeves that encircle the arm and are held in place with two adjustable Velcro straps. The patient wears the brace at all times and tightens the straps daily as swelling subsides. The brace may be removed upon clinical and radiographic signs of union, including less pain and bridging callus on radiographs (Figure 22.5). Active, self-assisted shoulder and elbow stretching exercises are initiated as comfort allows.
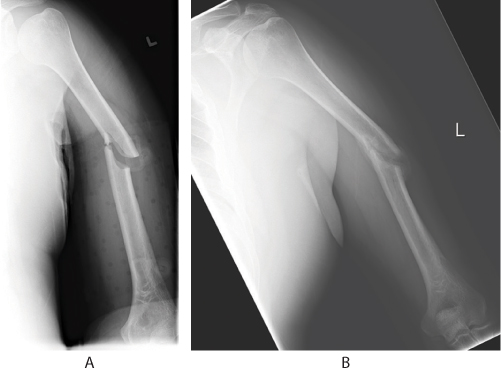
Figure 22.5 (a) Simple oblique fracture treated non-operatively in a functional brace. (b) Bridging callus with union at 10 weeks.
In Sarmiento’s largest case series of 620 humeral shaft fractures treated in a functional brace, over 80% healed in less than 16 degrees of varus and apex anterior angulation, 17% had union with greater deformity and 3% developed a nonunion treated operatively.8 Shoulder and elbow motion recovered completely in 60% and 76% of patients, respectively. However, this was a young, urban patient population (mean age 36 years), and many patients were lost early in the recovery period (33%).
Other groups have reported 80–89% union of isolated diaphyseal humerus fractures treated non-operatively.11,14 Koch et al. report that shoulder and elbow motion at the time of union (mean 10 weeks, range 5–36 weeks) was symmetrical and normal for 59% and 88% of patients, respectively. They noted that patients 40 years and older were more likely to lose shoulder and elbow motion, especially external rotation.
The effect of fracture location on the rate of union is debated. Koch et al. found that six out of nine nonunions were transverse fractures, and that only 73% of transverse fractures achieved union without surgery.11,15,16 and 17 Alternatively, in a retrospective review of 32 humeral shaft nonunions treated with functional bracing, Ring et al. found that only 4 (13%) were transverse, whereas 27 (84%) were spiral or oblique.18 Of 32 nonunions, 17 involved fractures of the proximal third, whereas only 1 involved a fracture of the distal third of the humerus.
Neuhaus et al. demonstrated that fracture gap is an independent predictor of radiographic and clinical nonunion at 6 weeks; each incremental millimeter of gap on initial in-brace radiographs was associated with a 1.4-fold greater odds of nonunion.14
Rehabilitation
In patients treated non-operatively, pendulum exercises for shoulder mobility can be initiated immediately after application of a functional brace if desired, but there is no evidence that this increases final shoulder motion and they are painful and somewhat difficult to do. Active self-assisted wrist and hand range of motion begins immediately, and elbow motion is encouraged as pain subsides. Active and active self-assisted abduction and forward elevation of the shoulder are delayed until union is established.
Some orthopaedic surgeons advocate immediate application of a functional brace in the emergency department, without any period of coaptation splinting (Egol KA. Personal communication. From Wasterlain AS, New York, 2014). The primary advantage of this approach is patient comfort and independence, as coaptation splints are bulky and difficult to manage.
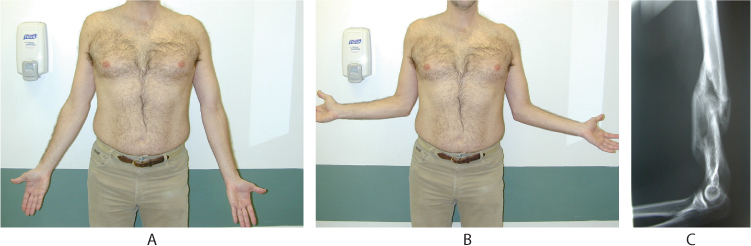
Figure 22.6 Patient with excellent functional outcome despite ‘malunion’ of greater than 30 degrees. Full and symmetric (a) extension and supination, and (b) external rotation of the affected (right) arm compared to the contralateral side. (c) Hypertrophic callus formation with bony union.
OPERATIVE TREATMENT
Indications
Open reduction and internal fixation (ORIF) is recommended for open fractures (except low velocity gunshot fractures), fractures associated with vascular injury and combined unstable fractures of the arm and forearm (the so-called ‘floating elbow’). Surgery is also considered in patients with multiple injuries to allow weight bearing of the affected arm for ambulation with assistive devices.
With respect to the fracture itself, shortening greater than 3 cm, rotation greater than 30 degrees and varus or apex anterior angulation greater than 20 degrees are sometimes cited as surgical indications, although malunion of any degree does not appear to affect function (Figure 22.6).19 Klenerman noted that despite preservation of limb function, cosmetic deformity becomes visible with apex anterior and varus angulation greater than 20 and 30 degrees, respectively,20 particularly in thin patients.
Most open fractures and high velocity gunshot wounds should be treated with irrigation and debridement in the operating room, followed by internal fixation. Fractures with intra-articular extension also benefit from surgery, as discussed elsewhere in this book. A fracture with overlying burns should be considered for operative treatment due to the increased risk of compartment syndrome, and because the skin condition may not be ideal for casting or bracing.
The risks and benefits of operative treatment must be discussed and the decision shared with each individual patient. Operative fixation typically permits earlier return to function, however it also carries the risk of nerve injury, infection, implant failure and other surgical complications. Options for operative fixation include plate osteosynthesis, intramedullary nailing and external fixation. Plating options and techniques include open reduction with conventional plates or locking plates and screws and minimally invasive plate osteosynthesis (MIPO).
At the time of writing there are very few high quality prospective studies comparing operative to non-operative treatment for humeral shaft fractures. A 2012 Cochrane review therefore concluded that no recommendations could be made for or against operative treatment for isolated closed diaphyseal fractures of the humerus.21 A prospective observational study conducted by the HUMMER group is currently underway to compare functional outcomes, measured by the Disabilities of the Arm, Shoulder and Hand (DASH) score, among operatively and non-operatively treated patients with humeral shaft fractures. In a retrospective comparison of functional bracing and compression plating, Denard et al. found no statistical difference in time to union or final range of motion of healed fractures.22 However, patients treated non-operatively were more prone to nonunion (21% vs 9%) and malunion (13% vs 1%).
Surgical approaches
The majority of humeral shaft fractures can be accessed and plated through an anterolateral or posterior approach. Less commonly, a direct medial or direct lateral approach may be used.
ANTEROLATERAL APPROACH
The anterolateral approach23 is ideal for plating proximal and middle third humeral shaft fractures. Advantages include easy patient positioning and the ability to extend the exposure proximally, with the disadvantage of a prominent scar. Distally, the approach and fixation construct must identify and protect the radial nerve and avoid the coronoid fossa.
The patient is placed in a supine or beach chair position. Prep the entire arm to permit extension of the approach as needed. The skin incision is centred over the fracture and may be extended proximally to the deltopectoral interval, following the lateral edge of the biceps and the anterior edge of the deltoid, and distally along the interval between the freely movable biceps muscle belly, stopping 5 cm proximal to the elbow flexion crease or crossing the elbow flexion crease obliquely when more distal exposure is helpful. The fascia over the biceps and brachialis is divided. Proximally, the plane between the deltoid laterally and the pectoralis major medially is identified by finding the cephalic vein and surrounding fat, which lie relatively superficial between these two muscles. The vein is usually kept medial but can be retracted either medially or laterally.
Proximally a plate will lie just lateral to the biceps tuberosity. The anterior part of the deltoid insertion is elevated to accommodate the plate. At the mid-diaphysis, the biceps is mobilized medially and the brachialis is split longitudinally along its fibers separating its lateral third (radial nerve) and its medial two-thirds (musculocutaneous nerve) (Figure 22.7). Elbow flexion relaxes the brachialis and facilitates dissection. The brachialis split is carried down to periosteum, and the muscle is reflected off the humerus, preserving the periosteum and as much muscle attachment as possible. The radial nerve is vulnerable as it traverses the spiral groove posteriorly in the mid-diaphysis, and as it lies between the brachioradialis and brachialis muscles distally in the anterior compartment. Use caution placing anterior-posterior screws mid-shaft and ensure that the nerve is not trapped under the distal lateral corner of the plate. An oscillating drill can help protect the nerve by avoiding the possibility of winding the nerve up in the drill.
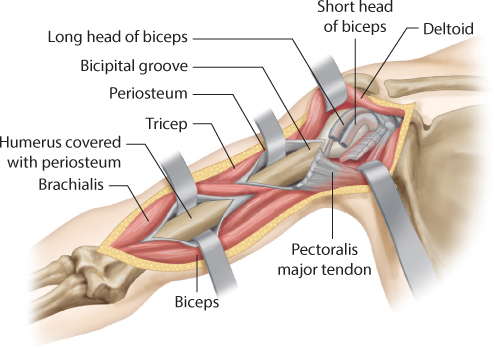
Figure 22.7 Anterolateral approach to the humerus. Proximally the interval is between the deltoid and pectoralis major muscles. The brachialis is split along its fibers at the mid-diaphysis.
POSTERIOR APPROACH
The posterior approach23 provides excellent exposure for fractures of the distal three-quarters of the humeral shaft and permits plating along the broad posterior surface of the humerus distally. Disadvantages are that the nerve is vulnerable intraoperatively and lies directly over the plate, and that prone or lateral positioning may be difficult in a polytraumatized patient.
The patient is placed prone or in the lateral decubitus position with the arm over a bolster. A tourniquet may be applied during the distal dissection and identification of the radial nerve, and then removed when working more proximally. The incision is centred over the fracture in the posterior midline and may be extended from the olecranon distally to the posterolateral aspect of the acromion proximally. The triceps muscle and fascia are divided sharply, taking care to identify and protect the radial nerve as it lies in the spiral groove of the humerus mid-shaft, and the profunda brachii artery, which travels with the nerve proximally. The approach continues proximally between the long and lateral heads of the triceps until the axillary nerve and posterior humeral circumflex artery are reached at the border of the deltoid (Figure 22.8a). If a plate is applied to the medial column of the distal humerus, identify and protect the ulnar nerve. The elbow joint can be accessed by performing an olecranon osteotomy and reflecting the triceps proximally.
MODIFIED POSTERIOR APPROACH
In the modified posterior approach described by Gerwin et al.,24 the lower lateral brachial cutaneous nerve, which branches off the radial nerve, is identified. The intermuscular septum is then divided deep to the lower lateral brachial cutaneous nerve, extending distally about 3 cm to reveal and permit mobilization of the radial nerve (Figure 22.8b). The medial and lateral heads of the triceps are elevated off the lateral intramuscular septum and swept medially, permitting exposure of up to 94% of the humeral diaphysis, compared to only 76% with a posterior triceps-splitting approach.
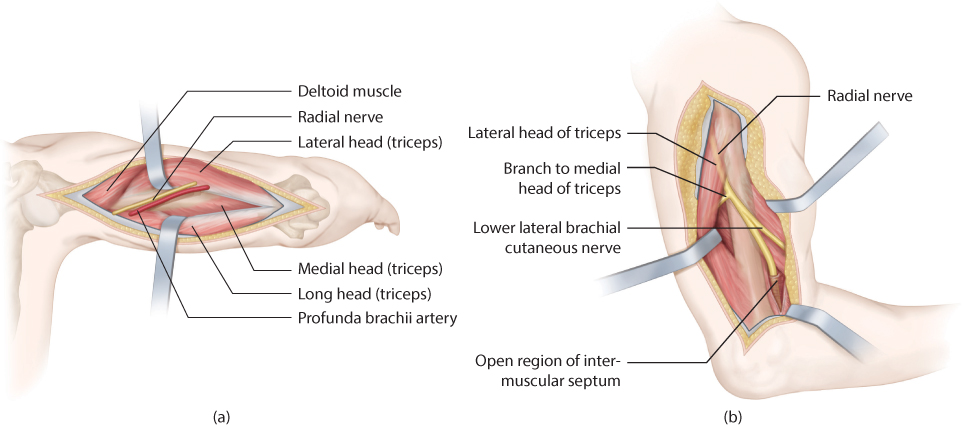
Figure 22.8 (a) Posterior approach to the humerus. The medial head of the triceps is divided sharply, taking care to protect the radial nerve and profunda brachii artery proximally. (b) Modified posterior approach to the humerus.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


