Metacarpal fractures
INTRODUCTION
Elderly patients with metacarpal fractures have thinner cortices and a higher likelihood of fixation failure. On the other hand, the fractures are typically due to low energy injuries and may less frequently benefit from fixation. Older patients often have lower functional demands and are more accepting of deformity. Preserving independence in an older person with a metacarpal fracture means avoiding cumbersome methods of hand immobilization.
EPIDEMIOLOGY
The annual incidence of hand fractures ranges from 61 per 10,000 people younger than 20 years of age to 29 per 10,000 people older than 20 years of age and from 37 per 10,000 males to 13 per 10,000 females.1,2 After age 65, women are at greater risk than men likely due to osteoporosis.3 More than a third of metacarpal fractures involve the small finger.3
CLASSIFICATION
There is no well-accepted or widely used classification system for metacarpal fractures. The AO/OTA universal fracture classification system can be applied to the metacarpals but has an interobserver kappa coefficient of 0.44 and an intraobserver kappa coefficient of 0.62.4 To permit comparison between study cohorts and facilitate communication between providers, metacarpal fractures are largely categorized by the location within the bone combined with the pattern of the fracture. Further distinction is given to degrees of comminution, intra-articular extension and open fractures. Metacarpal fractures are commonly divided into head, neck, shaft and base. Head and base fractures are intra-articular injuries; neck and shaft are extra-articular. Shaft fractures can be grouped as transverse/short oblique and spiral/long oblique. Transverse/short oblique fractures tend to angulate in the sagittal plane, apex dorsal (Figure 28.1). Conversely, displacement of long oblique/spiral fractures is characterized more by axial shortening and rotational deformity than sagittal plane angulation (Figure 28.2). At first glance, it can be difficult to distinguish a spiral from a long oblique fracture, but a spiral fracture always has one component of the fracture interface that runs in a pure longitudinal direction. The importance of distinguishing the two patterns relates simply to predicting the likelihood of malrotation, which is theoretically greater for the spiral fracture induced by a rotational mechanism of injury as opposed to the axial shearing mechanism of the long oblique fracture.
TREATMENT
Clinical evaluation
Comorbidities and activity level are important considerations in the elderly. Details about social support and living situation relate directly to the elderly patient’s capacity for self-care with an injured hand, the degree to which different types of splints may interfere with function and the availability of transportation to receive associated care such as hand therapy.1 Specific attention should be given to the mechanism of injury, including the direction of the applied force and the level of energy imparted, as this information will be used to estimate the probability of further displacement when selecting treatment.
Although shortening, translation and angular deformity can all be easily discerned on radiographs, axial rotation of the metacarpal is more difficult to evaluate. Ask the patient to actively flex the metacarpophalangeal (MP) joints as far as possible and examine the alignment of the digits relative to each other, viewing down the axis of the metacarpals (Figure 28.3). Axial malrotation of the metacarpal will cause the involved proximal phalanx to project radially or ulnarly, out of alignment with neighbouring digits. The often cited examination of nail plate alignment is unreliable for evaluation of axial rotation. The inherent stability of the fracture can be assessed by asking the patient to actively flex and extend within her comfort zone.
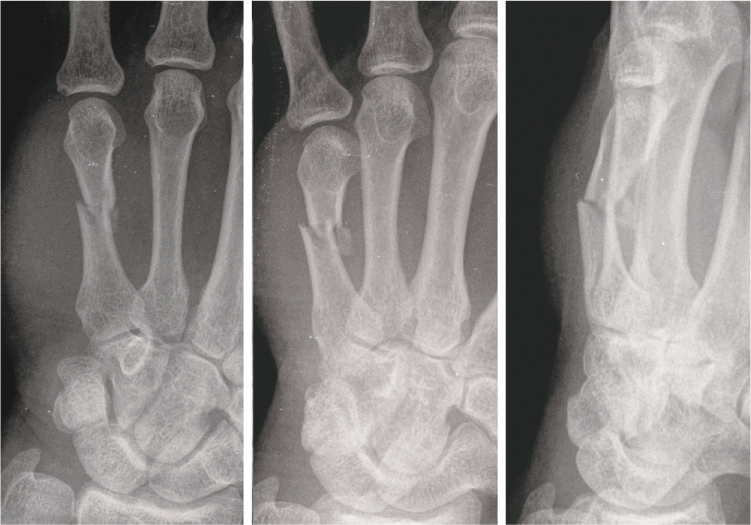
Figure 28.1 Transverse/short oblique fractures of the metacarpal shaft tend to angulate apex dorsal rather than shorten or axially rotate in comparison to long oblique/spiral fractures. The features of translation and the volar third fragment indicate a higher degree of inherent instability and periosteal disruption in this 68-year-old male.
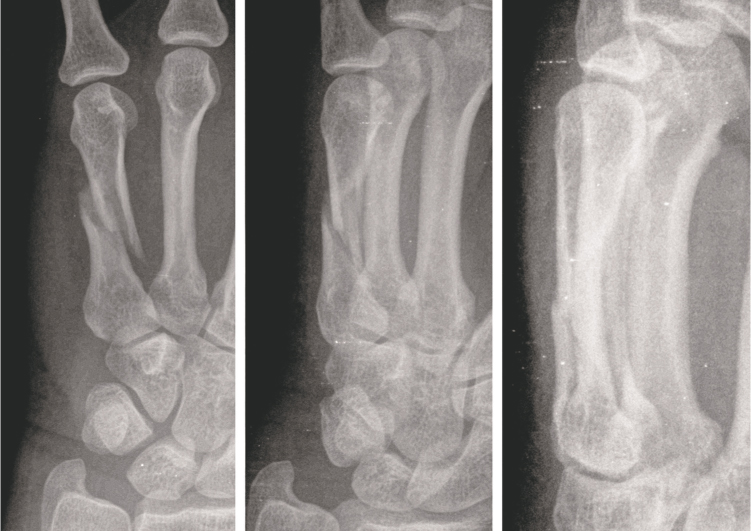
Figure 28.2 Spiral/long oblique fractures of the metacarpal shaft tend to shorten and axially rotate rather than angulate in the sagittal plane in comparison to transverse/short oblique fractures.
Excessive axial shortening or apex dorsal angulation at the fracture site theoretically poses the long-term threat of functionally limiting extensor lag. In cadaver studies, each 2 mm of axial shortening produced a corresponding 7 degrees of extensor lag.5 Reduced flexor efficiency has also been cited for angulations over 30 degrees at the small metacarpal neck.6,7 These cadaveric observations have not been borne out in clinical practice. A study of 42 patients with initial extensor lag from shortening all corrected the deficit by 1 year and achieved 94% of contralateral grip strength.8

Figure 28.3 Malrotation at the metacarpal level is best assessed by flexing the metacarpophalangeal (MP) joints and viewing down the axis of the metacarpal. The projection of the proximal phalanges (parallel or divergent) represents the rotation status of the metacarpal.
Radiographic evaluation requires at least three different views of the hand (Figure 28.4). The standard anteroposterior (AP) view is useful for evaluating relative shortening and revealing sagittal fracture planes. Oblique coronal fractures without translation or angulation are easily obscured on the AP view by fragment overlap and are better visualized on the oblique. A true lateral view offers little useful information at the head or shaft level as the metacarpal shadows overlap each other. If the lateral view is slightly supinated, it can at least show the index and long finger carpometacarpal (CMC) joint profile and rule out fracture dislocations. The most broadly useful third view is an oblique, pronated around 35 degrees. This gives sufficient pronation to overcome the problem of overlap seen on the lateral, but still facilitates reasonably accurate measurement of sagittal plane angulation and demonstrates the CMC profiles of the ring and small fingers.9 Multiple specialty views have been described but are rarely necessary.
Treatment planning
There are three categories of metacarpal fracture treatment: non-operative, closed reduction and pinning, and open reduction with internal fixation (ORIF). The non-operative category ranges from no immobilization of any kind to hard splints or casts spanning forearm to hand. In between are multiple designs for strapping or splinting that attempt to provide comfort and influence the position of the fracture while allowing motion. The pinning category includes transverse pinning to adjacent metacarpals, intramedullary pinning with one or more wires and interfragmentary/intrafocal pinning at the fracture interface. ORIF potentially includes any type of fixation device but, with modern systems, is largely confined to screws alone or plate and screws (Figure 28.5). The most successful outcomes result from matching the individual fracture and patient characteristics to the treatment strategy.10 Several differences between elderly and younger adult patients are worth considering:

Figure 28.4 Characteristic features of small finger metacarpal neck fracture demonstrating: (a) shortening and radial translation of the distal fragment on posteroanterior (PA) view, (b) apex dorsal angulation, volar impaction of the neck and supination deformity seen best on the oblique view and (c) apex dorsal deformity, volar translation and neck impaction and the extension proximally into the shaft best seen on the lateral view.
Cortical thickness is reduced, limiting the purchase of both Kirschner wires (K-wires) and screws, but with a greater relative impact on screws.
Cortical bone is weaker and more likely to fail adjacent to an implant, propagating new fracture lines from the point of implant penetration to nearby fracture edges or other implants.
Fixed angle screws near a joint can cut out of osteoporotic cancellous bone.
The adjacent small joints, MP and proximal interphalangeal (PIP) may have deformity and reduced motion from pre-existing osteoarthritis.
Infirm older patients may benefit from independent exercises when it is difficult to get to a hand therapist’s office.
Less active elderly patients may accept more deformity and stiffness than healthier, more active patients. Older generations may also be more adaptive.
Elderly patients with metacarpal fractures may be less prone to stiffness, perhaps due to relatively low energy injuries and diminished scarring.
Comorbidities such as coronary artery disease, congestive heart failure and chronic obstructive pulmonary disease increase the risks of anaesthesia.
Comorbidities such as diabetes and peripheral vascular disease may increase the complications of surgery.
Older patients may have lower physiological reserve when adverse events occur.
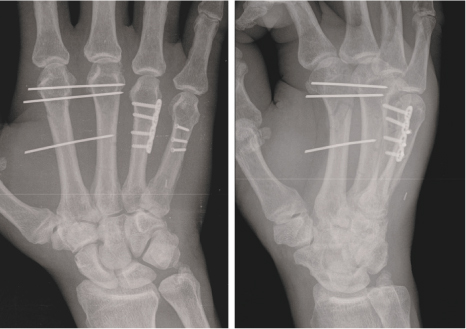
Figure 28.5 A very active working man with metacarpophalangeal (MP) osteoarthritis sustained heavy crush trauma with multiple metacarpal fractures (open at the ring finger, and small and closed at the index finger). Mixed fixation methods, tailored to match the fracture characteristics and associated soft tissue injuries, allowed immediate therapy that yielded a final result of range of motion (ROM) equivalent to contralateral. No one method of fixation is universally superior to another; the selection should simply correlate the advantages and disadvantages with the clinical features of the injury pattern.
Non-surgical treatment
Non-surgical treatment is appropriate for fractures with acceptable alignment and fractures that can be reduced to an acceptable position, provided that position can be effectively maintained. The most difficult displacement to reduce and control is translation and angulation in the coronal plane. High degrees of axial malrotation can be improved by neighbour strapping (particularly for the long and ring fingers) but cannot be reliably controlled without direct bony fixation. Sagittal plane translation and angulation is easily reduced but often tends to gradually drift back towards the position demonstrated in the original injury films.
Patients love to hear that the fracture will definitely heal. To decide if the alignment is acceptable to the patient, the surgeon can point out where prominences are expected, what the knuckle will look like and rotational deformity (especially when great enough to result in full digital overlap). Most patients, the elderly in particular, are unlikely to rate angular deformity or shortening displeasing enough to request more invasive treatment from a cosmetic standpoint alone. Once patients understand that the fracture will heal, the hand will function well and arthritis is not an issue, deformity is often quite acceptable.
The most relevant functional issue is an active extensor lag at the MP or PIP joint.5 If the patient does not demonstrate an extensor lag when acutely injured, then good final function can be anticipated without correction of the angular deformity or shortening. If a slight extensor lag is present acutely, correction through rebalancing after healing is anticipated.8 Rotational deformity is less well-tolerated but should be interpreted in the context of existing deformity patterns for the elderly hand. Subtle degrees that do not result in digital overlap are easy to adapt to. A moderate degree of initial rotational abnormality can be reduced and maintained by the influence of adjacent digits, particularly the long or ring finger.
If non-surgical treatment has been selected, the next decision concerns the method of immobilization or positional control. If the presenting posture is considered acceptable and no formal reduction was performed, then there is little need for splinting. Patients fare well with early motion, using side strapping for rotational control and prevention of catching the injured digit on clothing and furniture.11
If an unstable metacarpal fracture was reduced, then the patient may benefit from 3–4 weeks of initial intrinsic plus splinting.12 The MP joints are flexed around 70 degrees with the distal extent of the hard splint terminating at the level of the PIP joints, allowing full PIP motion. Hand based intrinsic plus splints are smaller and lighter to wear, but without the wrist support, some patients tend to flex the wrist, which drives MP extension and PIP flexion, counteracting the intended benefits of intrinsic plus splinting (Figure 28.6). Flexion of the MP joints reduces flexor and intrinsic tone and theoretically the tendency to pull the distal metacarpal fragment into flexion. An MP extension block with active flexion of the PIP joints might also help guide the injured ray into better rotational alignment. It is not clear that earlier performance of motion exercises necessarily achieves better final motion or alignment.13
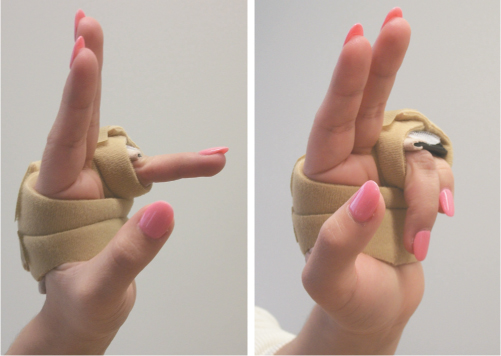
Figure 28.6 When a hard splint (intrinsic plus) is judged to be necessary, treatment related morbidity can be minimized by including only the fractured digit and its neighbour, allowing freedom of proximal interphalangeal (PIP) and wrist motion (provided the patient lacks the guarding response that encourages a wrist flexion posture).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


