Fig. 1
Intraoperative photo demonstrating patient setup following prepping and draping for a right hip arthroscopy. The right leg is in traction with the left leg abducted approximately 60°. The c-arm is positioned between the legs to aid in the establishment of portal placement as well as acetabular and cam lesion resection
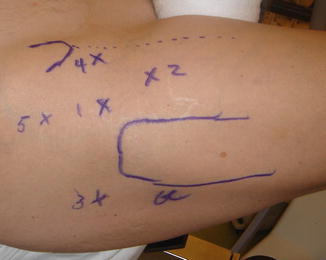
Fig. 2
Intraoperative photo showing provisional skin markings for portal placement. The anterior superior iliac spine (ASIS) and the greater trochanter are marked with a dashed line extending distally from the ASIS. The portals are (1) anterolateral, (2) mid-anterior, (3) posterolateral, (4) anterior, and (5) proximal anterolateral
Some prefer to “vent” the hip prior to prepping and draping to eliminate the vacuum phenomenon created with the leg in traction. This is done for two main reasons: (1) to assure the hip can be adequately distracted and (2) to reduce the amount of force necessary to distract the hip [13] This involves placing the leg in traction and, using sterile technique and fluoroscopy , placing an 18-gauge 6-in. spinal needle at the location of the anterolateral portal (see below). The needle is introduced with the long end of the bevel away from the femoral head to reduce articular cartilage gouging. The path of the needle is such that the tip of the needle should end at the upper portion of the cotyloid fossa and the junction of the medial most aspect of the sourcil, with the shaft of the needle next to the femoral head. When the tip of the needle is in the correct location within the central compartment, the stylus is removed (Fig. 3a, b) to eliminate the negative intra-articular pressure created by the joint distraction. While confirming the air arthrogram with the fluoroscope, one will also notice the relaxation of the quadriceps muscle as air initially enters the joint, indicative of relaxation of the capsule and its proprioceptive mechanoreceptors.
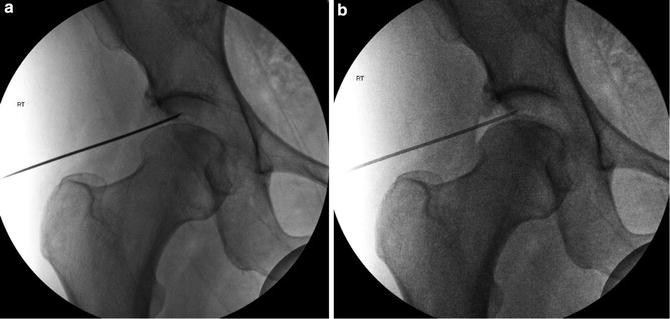
Fig. 3
(a) Fluoroscopic image of spinal needle used for localization of initial anterolateral portal following joint distraction. Note the trajectory of the needle adjacent to the femoral head (versus the acetabulum) so as to avoid penetration of the labrum. (b) Fluoroscopic image of spinal needle following removal of the stylus demonstrating the air arthrogram created and indicating intra-articular placement of the needle
Portal Overview
Hip arthroscopy portals utilized for working within the central compartment, peripheral compartment, and peritrochanteric space will be described. Most surgeons prefer two or three portals for standard hip arthroscopy involving the central and peripheral compartment.
The greatest risk in portal placement includes injur y to neurovascular structures as well as iatrogenic injury to the cartilage and labrum . The structures at greatest risk will be discussed individually with each portal description. The most recent literature indicates major and minor complication rates following hip arthroscopy of 0.6 % and 7.5 %, respectively, with complications specifically related to portal placement of 0.5–0.6 % [12, 14].
Anterolateral Portal
Placement
The anterolateral portal is typically the first portal established as it lies most centrally in the safe zone for hip arthroscopy. Positioning of the other portals within the central compartment is facilitated by viewing through this portal. The closest structure is the superior gluteal nerve at an average of 4.4 cm proximal [15]. The entry point on the skin is adjacent to the anterior-superior border of the greater trochanter. Under fluoroscopic guidance (Fig. 3a, b), a 6-in. 18-gauge spinal needle is directed through the gluteus medius muscle belly at approximately 15° cranially and 20–30° posteriorly to position the tip of the needle close to the femoral head. These are just general guidelines, as femoral version, femoral neck length, and neck-shaft angle vary. Another technique to identify the starting position and cranial-caudal angle is to overlay the needle on the skin. Using fluoroscopy , the needle is positioned to determine the skin entry point and angle of inclination by overlying the tip of the needle at the junction of the cotyloid fossa and sourcil, having the shaft of the needle next to the femoral head. Following the length of the needle to the skin will identify where the entry point should be along the length of the femur.
Fluoroscopy (the needle should be adjacent to the femoral head – Fig. 3a) and tactile sensation are utilized to avoid piercing the labrum with the spinal needle as subsequent placement of the trocar in this position will damage the labrum [13]. While minimal resistance is provided by the gluteus medius muscle belly, the hip capsule is a thick structure and provides greater resistance to needle penetration. Once the tip of the needle has penetrated the capsule, resistance should again be minimal as it enters the space of the central compartment. Again, the long end of the bevel of the needle should be away from the femoral head. Continued resistance will be experienced if the needle pierces the labrum or comes in contact with the femoral head or acetabulum.
The stylus of the spinal needle is then removed and a nitinol guide wire is placed through the needle. Leaving the guide wire in place, the needle is removed and a cannula with a cannulated obturator is placed over the guide wire. Some prefer to dilate the soft tissue around the portal with progressively larger obturators for easier placement of the final cannula (Fig. 4). After a second portal is established within the central compartment (the senior author prefers to create the mid-anterior portal next), a 70-degree arthroscope is inserted through this second portal to confirm appropriate placement of the anterolateral portal between the femoral head and acetabulum with avoidance of the labrum. If the anterolateral portal needs to be adjusted, this can be done with a spinal needle under direct visualization through the second portal.

Fig. 4
Fluoroscopic image of a cannula (with guide wire still in place) inserted into the anterolateral portal over a guide wire
Utility
Using a 70-degree arthroscope through the anterolateral portal, most of the structures within the central compartment can be visualized. Nearly the entire acetabular labrum can be seen; however, this portal provides the best visualization to the anterior and superior portions of this structure (Fig. 5). The articular cartilage surfaces of the femoral head and posterior-medial acetabulum are also well visualized (Fig. 6). Other structures that can be seen best through this portal are cotyloid fossa and ligamentum teres (Fig. 7), capsular-labral recess, and anterior triangle (Fig. 8). The anterior triangle is made up of the intra-articular portion of the iliofemoral ligament and capsule, the anterior superior portion of the femoral head, and the acetabular labrum. Visualization of this structure is particularly important as it allows for direct viewing of the spinal needle for creation of the anterior and/or mid-anterior portals.
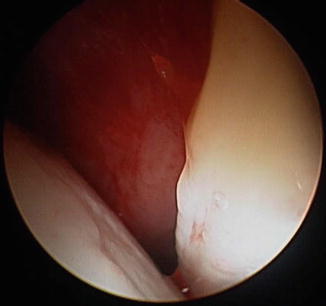
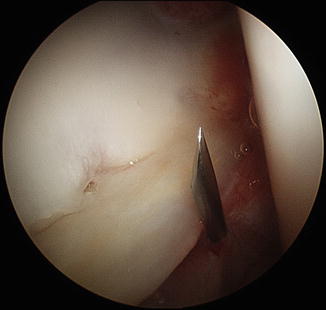
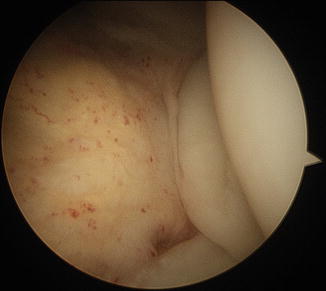
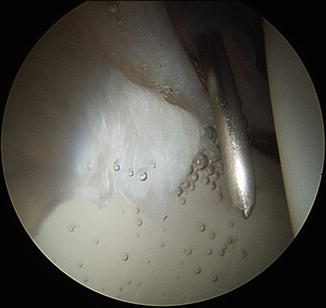
Fig. 5
Arthroscopic image with a 70-degree arthroscope of initial view through anterolateral portal showing the anterior-superior labrum on the right, femoral head on the left, and capsuloligamentous structure centrally
Fig. 6
Arthroscopic image with a 70-degree arthroscope from the anterolateral portal demonstrating spinal needle localization of the posterolateral portal. The acetabular cartilage and labrum can be seen on the left and the femoral head articular cartilage on the right
Fig. 7
Arthroscopic image with a 30-degree arthroscope from the anterolateral portal demonstrating the cotyloid fossa on the left, ligamentum teres centrally, and the femoral head on the right
Fig. 8
Arthroscopic image with a 70-degree arthroscope from the anterolateral portal showing needle localization of the mid-anterior portal through the anterior triangle. The anterior-superior labrum is on the left, femoral head is on the right, and the needle is piercing the capsuloligamentous structure
The anterolateral portal can also be used to work and/or visualize within the peripheral compartment of the hip. To access this compartment, traction is released and the camera is placed through the anterolateral portal at the junction of the femoral head and neck. Fluoroscopy can be useful to confirm the correct location. The femoral neck and anterior and superior aspects of the non-articulating portion of the femoral head can be visualized for eventual cam resection.
Related posts:
 Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Surgical Technique: Arthroscopic Treatment of Chronic Slipped Capital Femoral Epiphysis
Smith-Petersen Approach to the Hip
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Surgical Technique: Arthroscopic Treatment of Chronic Slipped Capital Femoral Epiphysis
Smith-Petersen Approach to the Hip
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


