Fig. 1
(a, b) AP pelvis radiograph with bilateral gluteus medius calcific tendonitis. Corresponding arthroscopic view demonstrating evacuation of the calcific deposit
This chapter describes the evaluation of the lateral aspect of the hip, the peritrochanteric space anatomy, the associated pathologic entities, and the endoscopic techniques used to effectively address them.
Anatomy of the Peritrochanteric Compartment
An understanding of the relevant anatomy of the trochanteric space is requisite for treating associated pathology. The peritrochanteric compartment is an anatomic region of the lateral aspect of the hip between the borders of the greater trochanter and iliotibial band (ITB) comprising the trochanteric bursa. Anteriorly, the compartment is bordered by the proximal sartorius and tensor fascia latae musculature. Medially, its limits are defined by the gluteus medius and minimus superiorly, extending distally past the vastus ridge to include the vastus lateralis. The lateral border is comprised of the fibers of the iliotibial band, and the peritrochanteric compartment terminates distally at the level of the gluteal sling insertion.
The greater trochanter has four distinct facets consisting of the anterior facet, superoposterior facet, lateral facet, and posterior facet. The gluteus minimus can be divided into a lateral and medial portion. The lateral portion arises from the superficial muscle belly and contains the main tendinous insertion on the anterior facet (Fig. 2), while the medial portion inserts on the anterior and superior capsules of the hip joint. The gluteus medius is comprised of an anterior, lateral, and posterior portion. The strong posterior portion inserts on the posterosuperior facet, while the lateral portion inserts distally on the lateral facet (Figs. 3 and 4). The anterior portion is mainly muscular and joins the gluteus minimus tendon interiorly [13].
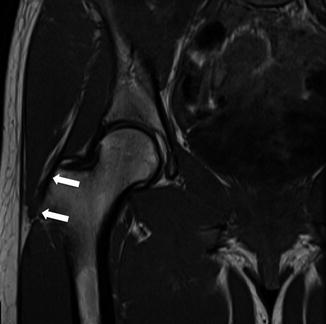
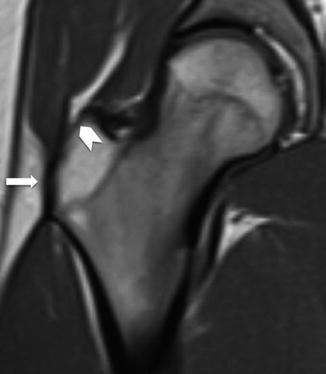
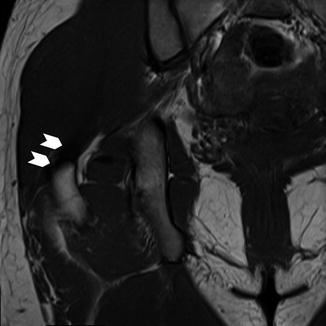
Fig. 2
Coronal T1-weighted MRI image showing the normal gluteus minimus tendon (arrows) inserting on the anterior facet of the greater trochanter
Fig. 3
Coronal T1-weighted MR image in a patient with a normal gluteus medius tendon. The lateral part of the gluteus medius tendon (arrow) inserts at the lateral facet of the greater trochanter. The open arrowhead points to the trochanteric bald spot
Fig. 4
The main portion of the normal gluteus medius tendon (arrow heads) inserts on the posterior superior facet of the greater trochanter
Three distinct bursas are consistently present in most individuals, although bursa anatomy can be variable. The trochanteric bursa encompasses the posterior facet of the greater trochanter and is typically the largest bursa encountered. The subgluteus medius bursa lies between the superior portion of the lateral facet and the lateral portion of the gluteus medius tendon. The subgluteus minimus bursa lies beneath the gluteus minimus tendon medial and superior to its insertion [14].
Endoscopic Techniques
There is certainly an improved understanding of hip pathology given the advancements in hip imaging and surgical techniques. Specialized arthroscopic hip instrumentation has enabled surgeons to access the hip and perform procedures that were once only possible with open techniques. Voos et al. [12] described disorders of the peritrochanteric hip and an endoscopic technique to address this extra-articular compartment.
In most individuals, the intra-articular compartment is first inspected to assess for concomitant hip pathology prior to examining the peritrochanteric space. With this completed, attention is directed to the extra-articular spaces. It is important to understand the anatomy of the peritrochanteric compartment. The borders consist of the iliotibial band and tensor fascia lata laterally, vastus lateralis inferomedially, abductor tendons superomedially, gluteus maximus muscle superiorly, and gluteus maximus tendon insertion on the linea aspera posteriorly. Within this space, the trochanteric bursa can be found.
A consistent, routine endoscopic evaluation assures that all pathology is addressed. Examination of the space is generally performed through three portals, although portal placement for the peritrochanteric space can vary among surgeons.
Once the procedures in the central and peripheral compartments are completed, the leg is positioned in full extension, held in 0° of adduction and 10–15° of internal rotation. The first portal is the mid anterior (MA) portal, which is used to first establish access to the peritrochanteric space (Fig. 5). The portal is placed 1 cm lateral to a line extending distally from the anterior superior iliac spine (ASIS) in the soft spot interval between the tensor fascia latae and sartorius. The cannula is directed into the peritrochanteric space with the tip directed toward the vastus ridge and the cannula swept between the iliotibial band and the greater trochanter once in the peritrochanteric space. This technique is analogous to accessing the subacromial space in the shoulder where the iliotibial band is analogous to the undersurface of the acromion. When the portal is placed appropriately, a clear space lying between the iliotibial band and the greater trochanter can be easily identified. If in doubt, the cannula should be placed directly lateral to the greater trochanter and confirmed on fluoroscopy if needed (Fig. 6). A second, anterolateral (AL) portal is utilized just proximal to the tip of the greater trochanter. This portal is similar to the standard anterolateral portal established for central compartment visualization. This is utilized as a proximal working portal and can also be utilized to visualize distally. A third, distal anterolateral accessory (DALA) portal is used for diagnostic evaluation and operative intervention. The distal anterolateral portal is placed in line with the proximal anterolateral portal. If standard portals do not allow clear access to the peritrochanteric space, further portals can be established for visualization and instrumentation. Spinal needle localization can assist in obtaining the correct positioning of these portals. Oftentimes, these three portals are the same portals utilized for intra-articular compartment access.
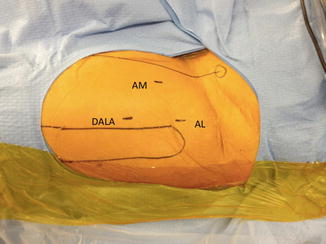
Fig. 5
 Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Surgical Technique: Arthroscopic Treatment of Chronic Slipped Capital Femoral Epiphysis
Smith-Petersen Approach to the Hip
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Surgical Technique: Arthroscopic Treatment of Chronic Slipped Capital Femoral Epiphysis
Smith-Petersen Approach to the Hip




Portals for peritrochanteric space access: AL antero lateral, MA mid-anterior, DALA distal antero lateral accessory
Related posts:
Athletic Populations of Interest in Hip Arthroscopy and Hip Preservation Surgery
Nerve Injuries Around the Hip
Selective and Image Guided Injections Around the Hip and Pelvis
Surgical Technique: Resection Arthroplasty
Surgical Technique: Arthroscopic Treatment of Chronic Slipped Capital Femoral Epiphysis
Smith-Petersen Approach to the Hip
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
