Fig. 1
T-capsulotomy perpendicular to interportal capsulotomy
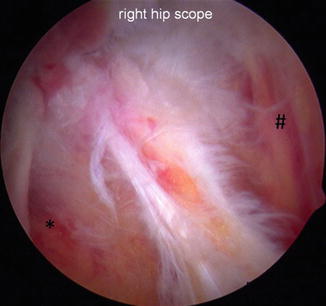
Fig. 2
Interval of the iliofemoral ligament between gluteus minimus (*) and iliocapsularis (#)

Fig. 3
Vertical incision through the iliofemoral ligament (IFL)

Fig. 4
Completed T-capsulotomy to expose the cam deformity
Once the capsulotomy is complete, a switching stick is introduced in the ALP (Fig. 5). The switching stick is used as a retractor of the superior and inferior leaflets of the capsule to improve visualization of the cam lesion (Fig. 6). Fluoroscopic images taken at a 45° angle to obtain a Dunn lateral view of the hip are frequently utilized to assess the extent of the cam lesion and retractor placement. The arthroscopic burr is inserted through the DALA portal for cam resection in a more ergonomic position (Fig. 7).

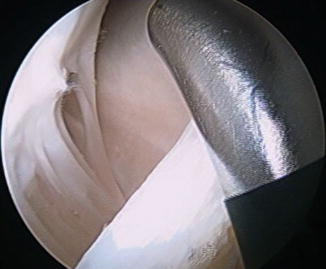

Fig. 5
Switching stick through the anterolateral portal (ALP) to retract the lateral leaflet of the iliofemoral ligament (IFL) and burr through the DALA portal
Fig. 6
Retraction of the medial leaflet of the iliofemoral ligament (IFL) to expose the medial synovial fold
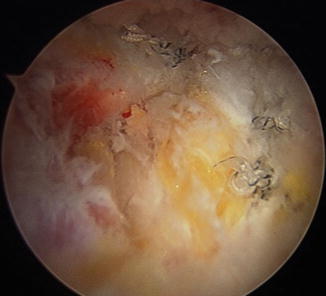
Fig. 7
Cam lesion preparation
Improved exposure superior and inferior can be obtained with repositioning of the switching stick either above or below the femoral neck (Figs. 8 and 9). Increasing hip flexion angle to 45° allows improved access to the distal femoral neck for larger cam lesions and visualization of the entire osteochondroplasty. Rotation of the hip in conjunction with fluoroscopic images helps improve access to anterior and posterior extents of the cam lesion (Fig. 10). This technique provides at least 180° visualization of the cam lesion and osteochondroplasty without extensive capsulectomy (Table 1).



Fig. 8
Retraction of the medial leaflet to expose the anteromedial cam
Fig. 9
Retraction of the lateral leaflet to expose posterolateral cam
Fig. 10
View showing lateral extent of cam lesion
Interportal capsulotomy | Provides adequate visualization and mobilization in the central compartment |
|---|---|
T-capsulotomy | Provides adequate visualization to fully evaluate the proximal femur |
Arthroscope in anterior portal | Directing the light source down the femoral neck allows at least 180o visualization of the cam lesion |
Retraction | (1) Switching stick through the anterolateral portal to retract the medial and lateral leaflets of the capsule for improved exposure |
(2) Traction sutures in each limb | |
DALA portal | Allows ergonomic osteochondroplasty of the femoral head-neck junction |
An alternative method of retracting the capsule is to place retraction suture in each leaflet (Fig. 11). The authors’ preferred technique for this is to place one suture in the medial limb near the proximal corner and to retrieve it through the DALA portal. Two sutures are placed in the lateral limb with one in the proximal corner and one at the base. These stitches are retrieved through the ALP. The sutures are then snapped with tension against the skin. The sutures are placed typically through a cannula in the DALA portal but can also be placed through the ALP. The sutures can also be used for repair after completion of the femoral osteochondroplasty. This technique allows access to approximately 90 % of most cam lesions and requires no additional surgical assistance.
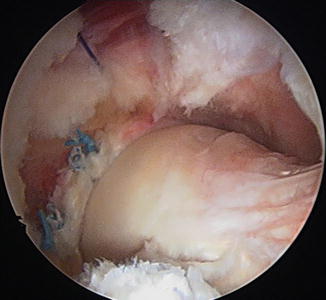
Fig. 11
Capsular suspension by placing retraction suture in each leaflet
After the femoral head-neck osteochondroplasty is complete (Fig. 12), a dynamic arthroscopic exam of the hip is performed (Fig. 13). The hip is flexed to 60° and rotated internally and externally, ensuring there is no impingement on the labrum, liftoff, or subluxation of the femoral head. Also the proximal extent of the cam resection should not violate the suction seal of the hip joint. Fluoroscopic images are used to assess anatomic recontouring of the femoral head-neck junction.
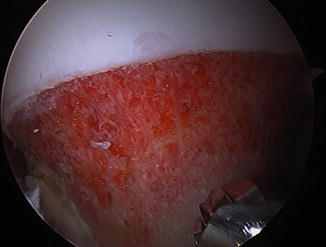
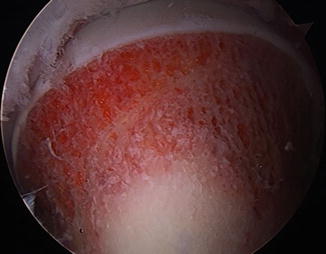
Fig. 12
Completed femoral osteochondroplasty
Fig. 13
Dynamic examination after completed femoral osteochondroplasty
We routinely repair the capsule after the capsulotomy. This is done with the arthroscope in the anterior portal, utilizing the same visualization as for cam osteochondroplasty. A cannula is introduced in the DALA portal. A commercially available suture-passing device designed for closure of the hip capsule allows for a single portal technique. It is introduced through the cannula, and a suture is passed through the medial and lateral capsule leaflets starting distally and working proximally. The knot is tied on the outside of the capsule through the DALA portal (Fig. 14). We have found that it typically takes three to four passes to adequately close the capsule to the level of the interportal capsulotomy and cover the femoral osteochondroplasty. The authors’ currently prefer to close the transverse capsulotomy. This is typically done through the ALP with two simple stitches. An alternative technique for capsular closure is to utilize a suture lasso technique. A suture passer is utilized through the DALA portal. The suture can be passed through the ALP and then tied through the DALA portal.
 Neuromuscular Hip Disorders: Focus on Cerebral Palsy
Neuromuscular Hip Disorders: Focus on Cerebral Palsy
 Femoral Deformities: Varus, Valgus, Retroversion, and Anteversion
Femoral Deformities: Varus, Valgus, Retroversion, and Anteversion
 Surgical Technique: Arthroscopic Labral Management
Surgical Technique: Arthroscopic Labral Management
 Surgical Technique: Endoscopic Gluteus Medius Repair
Surgical Technique: Endoscopic Gluteus Medius Repair
 Introduction to Static and Dynamic Overload of Hip Pathology
Introduction to Static and Dynamic Overload of Hip Pathology
 Atraumatic Instability and Surgical Technique
Atraumatic Instability and Surgical Technique




Related posts:
Neuromuscular Hip Disorders: Focus on Cerebral Palsy
Femoral Deformities: Varus, Valgus, Retroversion, and Anteversion
Surgical Technique: Arthroscopic Labral Management
Surgical Technique: Endoscopic Gluteus Medius Repair
Introduction to Static and Dynamic Overload of Hip Pathology
Atraumatic Instability and Surgical Technique
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
