I. Cervical Spine
A. Clinical Anatomy
1. Occipitoatlantoaxial complex—The cervical spine consists of two atypical vertebrae, the atlas (C1) and axis (C2), and five lower cervical vertebrae. The occipitoatlantoaxial complex functions as a unit, being composed of synovial joints surrounding the articulations and devoid of any intervertebral discs. The atlas consists of an anterior and posterior arch and two lateral masses. The superior surfaces of the lateral masses articulate with the occipital condyles, allowing 25° of flexion and extension and 5° of lateral bending and rotation. The inferior aspect of the lateral masses of C1 articulates with the superior facets of C2, allowing rotation. Approximately 50% of the rotatory movement of the entire cervical spine occurs at the atlantoaxial articulation. In the upper cervical spine, flexion is limited by bony anatomy, and extension is limited by the tectorial membrane. Rotation and lateral bending are restricted by the contralateral alar ligament. The axis, or second cervical vertebrae, consists of a vertebral body, an odontoid process (dens), pedicles, laminae, and a spinous process. The synchondrosis between the dens and the body of the axis generally closes by age 6 years, but may persist into adulthood as a thin sclerotic line that may resemble a nondisplaced fracture.
2. Odontoid process—The odontoid process (dens) with its attached ligamentous structures is the major stabilizer of the atlantoaxial articulation. The atlantoaxial joint depends on a complex of ligaments for stability (Fig. 26-1). The dens is held against the anterior arch of the atlas by the strong transverse ligament, which inserts on the lateral masses of C1. The alar ligaments originate from the occipital condyles, attach to the tip of the dens, and limit excessive lateral flexion and rotation. The apical ligament originates at the ventral surface of the foramen magnum and inserts on the tip of the odontoid. It is only a minor stabilizer of the craniocervical junction. The odontoid may fracture alone or occasionally in combination with ligamentous disruption. Isolated rupture of the transverse ligament, although common in patients with rheumatoid arthritis, is relatively uncommon, secondary to trauma. At the C1–C2 level the space available for the spinal cord is greater than at any other level of the cervical spine. Steel’s rule of thirds states that the area inside the atlas is equally occupied in thirds by the dens, spinal cord, and space. The space is primarily occupied by cerebrospinal fluid. This accounts for the low incidence of spinal cord injuries associated with C1 and C2 fractures. Complete spinal cord injuries at this level are rarely survivable events.
3. Anatomy of the subaxial cervical spine—The subaxial cervical vertebrae (C3 to C7) are relatively uniform in their morphologic characteristics. The vertebral body is connected posteriorly to the neural arch by the pedicles. The pedicles connect the vertebral body to the lateral masses. Within the lateral masses are superior and inferior facets, which form diarthrodial joints. The facet joints are oriented 45° in the sagittal plane and neutrally in the coronal plane. The superior articular facet (of the lower vertebrae) is anterior and inferior to the inferior articular facet of the vertebra above. The uncinate processes are small, bony ridges that project from the posterolateral aspect of the superior end plate of the vertebral body. They articulate with indentations on the inferior surface of the adjacent vertebral body, which form the uncovertebral joints of Luschka. The transverse foramina from C2 to C7 are surrounded by the pedicles, transverse processes, and facets. Spinous processes from C2 to C6 are usually bifid. The C7 spinous process is usually nonbifid and the most easily palpable. The vertebral arteries originate from the first branch of the subclavian arteries and usually enter the spine at the foramen transversarium of C6. The artery passes through the foramen of C1 and then turns sharply medially and superiorly into the foramen magnum. Although rare, fractures of the transverse process or fracture-dislocations of the cervical spine may cause injury to the vertebral artery.
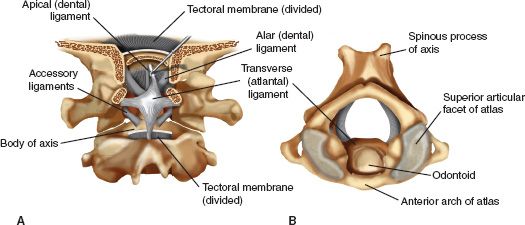
FIGURE 26-1 Atlantoaxial joint and cranium (the occipitoatlantoaxial complex). A. Posterior coronal view. Note the alar, transverse, and apical ligaments. B. Superior view of the atlantoaxial articulation.
4. Stability of the subaxial cervical spine—The lower cervical spine has little intrinsic bony stability. Spinal ligaments include the anterior and posterior longitudinal ligaments, the ligamentum flavum, and the supraspinous, interspinous, and intertransverse ligaments. The anterior longitudinal ligament covers the anterior surface of the vertebral body and resists extension moments to the vertebral column. The posterior longitudinal ligament is narrower than the anterior longitudinal ligament and is continuous with the tectorial membrane. It covers the posterior surface of the vertebral body and resists hyperflexion moments. The interspinous and supraspinous ligaments insert on the spinous processes and limit flexion. The intervertebral discs between the bodies of the vertebrae consist of a central nucleus pulposus and a strong outer annulus fibrosis, which also provides stability and limits motion at each level of the subaxial cervical spine.
B. Injuries of the Cervical Spine
1. Injuries involving the occiput, atlas, and axis
• Atlanto-occipital dislocation—Atlanto-occipital dislocation usually results from a high-energy injury in a patient with concomitant head trauma; the injury is often fatal. These rare injuries are often associated with significant delays in diagnosis.
• Occipital condyle fractures—Anderson and Montesano classified occipital condyle fractures seen on CT based on mechanism of injury.
(a) Type I injuries are impaction fractures of the condyle secondary to an axial load.
(b) Type II injuries are basilar skull fractures associated with fractures of the condyle.
(c) Type III injuries are avulsion fractures of the alar ligaments. This type of injury represents a more unstable injury with a higher association with atlanto-occipital dissociation.
• Atlas (C1) fractures—Atlas (C1) fractures are generally felt to be secondary to an axial load. Fracture of the C1 ring can involve the anterior arch, the posterior arch, the lateral masses, or most commonly the anterior and posterior arches (Jefferson’s fracture). Fractures of the atlas are usually not associated with neurologic symptoms and most are stable. Injuries are considered radiographically unstable if the open-mouth AP radiograph reveals a combined lateral mass step-off larger than 7 mm. This amount of step-off suggests rupture of the transverse ligament, the strongest and the most important ligament for stability between C1 and C2. Posterior arch fractures are usually the result of extension forces and are often associated with odontoid fractures or traumatic spondylolisthesis of C2.
• C1–C2 subluxation—C1–C2 subluxation resulting from acute transverse ligament rupture is rare and as with atlanto-occipital dislocation is often fatal. The mechanism is disruption of the transverse ligament with a resultant increase in the anterior atlantodens interval. According to Fielding, if there is less than 3 mm of anterior displacement the transverse ligament is intact; if there is 3 to 5 mm of anterior displacement the transverse ligament is ruptured; and if there is more than 5 mm of anterior displacement the transverse and alar ligaments are likely ruptured. Further, if the ADI is greater than 7 mm, there is probable rupture of the tectorial membrane.
• Atlantoaxial rotatory subluxation—Atlantoaxial rotatory subluxation is often difficult to diagnose, which may cause a delay in treatment. In adults, the injury is usually related to motor-vehicle trauma and may be associated with fracture of the lateral mass as a result of flexion and rotation. In children, the injuries are usually self-limited and are the result of a viral illness. Fielding divides rotatory subluxation into four types (Fig. 26-2).
(a) Type I injuries are the most common. Radiographic findings reveal fixed rotational deformities without anterior displacement or disruption of the transverse ligament.
(b) Type II injuries demonstrate transverse ligament insufficiency with 3 to 5 mm of anterior displacement of the atlas.
(c) Type III injuries have more than 5 mm of anterior displacement of the atlas. The transverse ligament is typically ruptured.
(d) Type IV injuries are the least common and include posterior displacement of the atlas and associated rotatory subluxation.
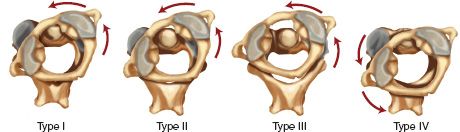
FIGURE 26-2 Four types of atlantoaxial rotatory subluxation according to Fielding.
• Odontoid fractures—Odontoid fractures may occur when flexion forces cause anterior displacement or when extension forces cause posterior displacement of the odontoid. These motions result in impingement of the dens against either the anterior arch of the atlas or the transverse ligament. The classification system most often used is that by Anderson and D’Alonzo (Fig. 26-3).
(a) Type I fractures are extremely uncommon and occur at the tip of the odontoid, probably as the result of avulsion of the alar ligaments. Type I fractures may be associated with craniocervical dislocation and must be ruled out radiographically and clinically.
(b) Type II fractures are the most common and occur at the junction of the base of the odontoid and the body of C2. The fracture does not extend into the C1–C2 articulation. Type II fractures have a high rate of nonunion and pseudoarthrosis because the blood supply to the cephalad fragment is disrupted.
(c) Type III fractures occur within the cancellous bone of the body of the axis.
• Traumatic spondylolisthesis of the axis—Traumatic spondylolisthesis of the axis (hangman’s fracture) is usually a combined hyperextension and axial loading injury, causing fracture of the C2 pars interarticularis. As with other fractures of the upper cervical spine, traumatic spondylolisthesis of the axis tends to decompress the neural canal, and thus neurologic involvement is uncommon. The most widely used classification is by Levine and Edwards and is based on a lateral cervical spine radiograph (Fig. 26-4).
(a) Type I fractures are usually secondary to hyperextension and axial loading with less than 3 mm of displacement of C2 on C3.
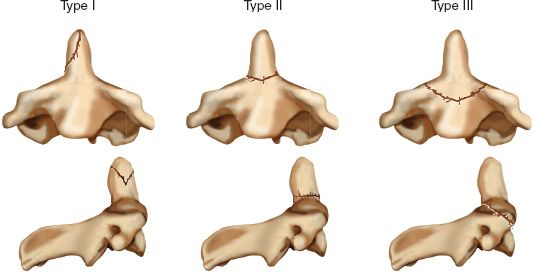
FIGURE 26-3 Anderson and D’Alonzo classification of odontoid fractures.
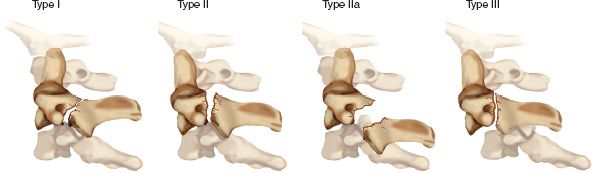
FIGURE 26-4 Classification of traumatic spondylolisthesis of the axis as described by Levine and Edwards.
(b) Type II injuries also result from hyperextension and axial loading but have significant angulation, translation, or both. Type IIa fractures are the result of a flexion force and have minimal translation but severe angulation.
(c) Type III fracture-dislocations are secondary to a flexion force and result in severe angulation and displacement as well as concomitant unilateral or bilateral facet dislocations at C2–C3. Type III injuries are the pattern most commonly associated with neurologic deficits.
(d) Stability—Type I fractures are stable, whereas Types II, IIa, and III are unstable disruptions of the C2–C3 motion segment.
2. Injuries involving the lower cervical spine—The lateral cervical spine radiograph is important to evaluate for gross bony or ligamentous injury by ensuring continuity of the longitudinal “lines” (Fig. 26-5). A comprehensive classification system of closed fractures and dislocations of the lower cervical spine based on mechanism of injury has been described by Allen and Ferguson (Fig. 26-6). This classification describes both the major injury vector and the position of the head and neck at the time of injury. There are six basic categories.
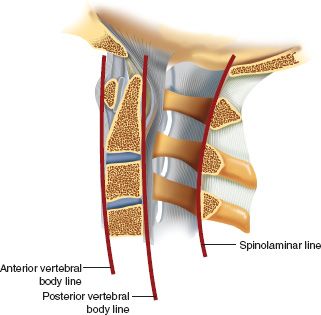
FIGURE 26-5 Radiographic lines seen on the lateral cervical spine film to evaluate for bony or ligamentous injury. The facets appear as stacked blocks or parallelograms.
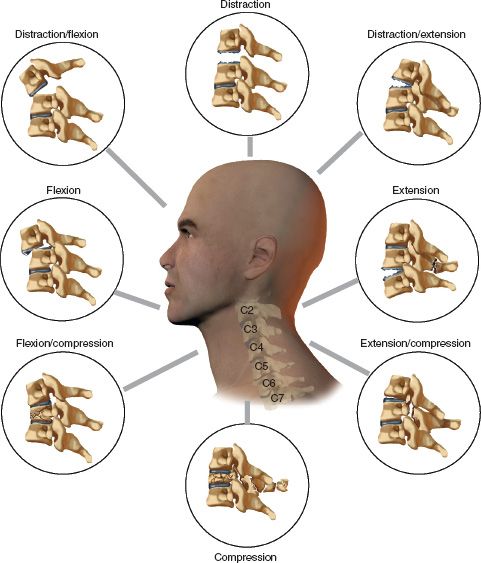
FIGURE 26-6 Mechanistic classification of fractures and dislocations of the lower cervical spine as described by Allen and Ferguson.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


