Proper application of imaging procedures is essential to obtain required information for diagnosis and therapy on patients with suspected calf, foot, and ankle pathology.1,2,3,4,5,6,7,8,9,10,11 Standard radiographic views that include anteroposterior and lateral standing and oblique views are essential and provide adequate screening for most skeletal abnormalities. Special views, such as fluoroscopically positioned spot films, are also useful because of the complex osseous anatomy of the foot and ankle. The American College of Radiology (ACR) Appropriateness Criteria rank imaging procedures for multiple conditions from 9 (most useful) to 1.11 Radiographs are ranked 9 as the initial screening study. Radionuclide studies can be valuable for detecting subtle skeletal lesions (ACR rank 1 in most cases), but have been largely replaced by cross-sectional imaging techniques.12,13,14 Computed tomography (CT) has provided valuable information regarding both osseous and soft tissue pathology in the calf, foot, and ankle. Ultrasound can be utilized to differentiate superficial soft tissue lesions and study abnormalities in certain tendons, especially the Achilles tendon.5,15,16,17,18,19 Ultrasound (ACR 8) is ranked just below magnetic resonance (ACR 9) for evaluation of tendon disorders. More invasive procedures such as arthrography, tenography, and angiography may also be required to evaluate the ligaments, tendons, and vascular structures.4,5 Ultrasound can also be used for image guided interventions in the foot and ankle.11,17,19
Applications for magnetic resonance imaging (MRI) of the foot and ankle disorders have expanded dramatically in the last decade.20 MRI is particularly suited to evaluation of the complex bone and soft tissue anatomy of the foot, ankle, and calf because of its superior soft tissue contrast and the ability to image in multiple planes. MRI is the recommended study for many conditions following initial radiographs.11 In addition, new fast scan techniques provide improved efficiency and allow motion studies to be performed. MR arthrography and angiographic techniques have improved significantly in recent years, resulting inmore routine use of these techniques.21
TECHNIQUES
Bone and soft tissue anatomy is complex in the foot and ankle. Axial, coronal, or sagittal images adequately demonstrate the anatomy in most clinical settings. However, positioning of the foot must be carefully accomplished so that the anatomy is not distorted. In some situations, off-axis oblique images may be required to optimally demonstrate anatomy.5,22,23,24,25 Technical considerations include magnet configuration, coil selection, patient positioning, pulse sequence selection, field of view, and matrix size and acquisitions.5,25 The basics of contrast media, indirect and direct arthrography, and MR angiography are discussed in Chapter 3.
Figure 8.1 Patient positioned for examination of the foot and ankle using flat (A) and circumferential (B) coils. The former allows more flexibility with positioning and motion studies. The circumferential coil provides more uniform signal intensity but reduces positioning options.
PATIENT POSITIONING AND COIL SELECTION
MRI can be accomplished at different field strengths and variable magnet configurations. Today, 1.5 or 3.0 T units are most commonly used. Conventional closed bore, open bore, and extremity units are also available. Patient positioning will vary depending upon the configuration of the MR unit.5,25 The patient should be studied with a closely coupled coil to achieve optimal signal-to-noise ratios and spatial resolution.2,4,5,20,25,26,27,28,29,30,31 Conventional surface coils take several configurations—flat, partial volume, or circumferential (Fig. 8.1). Different coils are suited to certain types of examinations. Generally, fine detail, circumferential volume coils or wrap-around coils are used for examination of the foot and ankle (Fig. 8.2). In certain cases, if comparison is needed, either dual coupled coils or the head coil can be used to reduce examination time.5,28,32 The extremity coil can be used to evaluate the calf.
Figure 8.2 Extremity (A) and high detail digital (B) coils used for foot and ankle imaging. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, Lippincott Williams & Wilkins; 2011.)
Patients can be examinedin the supine or proneposition, depending on which anatomic region is being studied.5,32,33 The prone position is useful for examination of the midand forefoot and assists in reducing inadvertent motion.5,32 Forefoot pathology, such as Morton neuroma, is more clearly displayed in this position.34 The prone position is also optimal for evaluating the posterior soft tissues of the calf. This avoids soft tissue compression that can distort the anatomy. However, the hindfoot soft tissues can be distorted when the patient is prone due to excessive plantar flexion of the foot (Fig. 8.3). For example, we prefer the supine position for patients with suspected Achilles tendon pathology. In this setting, it is best to have the patient supine with the foot in neutral position so that the tendons are not collapsed or buckled, which occurs when the patient is prone or the foot is in the plantar-flexed position (Fig. 8.3B). In some cases, dorsiflexion or plantar flexion may be required to evaluate fully the origin and/or insertion of the Achilles and other tendons about the ankle.5,32 Image quality may be improved by using more numerous (smaller degrees of plantar and dorsiflexion) positions. Farooki et al.35 used a positioning device to evaluate optimal positions for imaging the ankle tendons and ligaments. The peroneal tendons, extensor digitorum longus, and extensor hallucis longus were optimally imaged with the foot in 20° of plantar flexion and 20° of inversion. The calcaneofibular and anterior talofibular ligaments were optimally imaged with the foot in 20° of plantar flexion.35
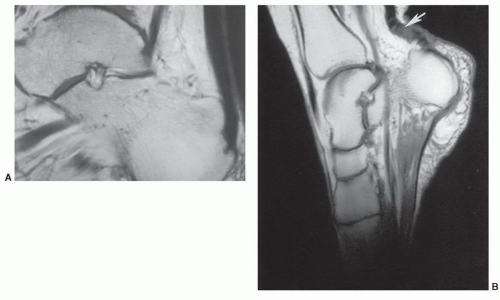
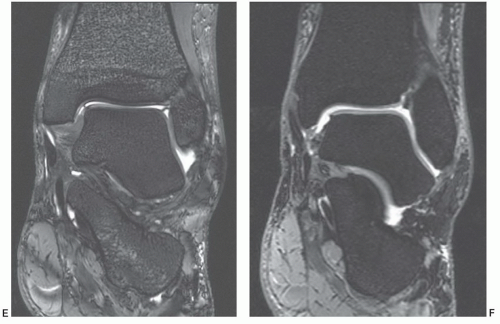
Figure 8.3 Sagittal T1-weighted MR images of the ankle with the foot in neutral position and the patient supine (A) and plantar flexed (prone) (B) positions. Note the buckling, partial volume effects of the Achilles tendon (arrow), and rotation of the calcaneus in B.
The foot and ankle should be supported with foam sponges and straps to prevent motion artifact when motion studies are not being performed. Motion studies are usually performed using flat or coupled coils.5,32 However, when dynamic studies are required, ultrasound may be the technique of choice.11,17
IMAGE PLANES
Coronal, axial, and sagittal image planes are commonly used for foot and ankle examination. In the foot, coronal images are perpendicular to the metatarsals and axial images in the plane of the metatarsals.5,20,32,33 To achieve patient comfort and to optimize image planes, oblique planes are frequently used in the foot and ankle.5,20,36,37 We generally use a minimum of two image planes at 90° angles to evaluate foot and ankle disorders. Figure 8.4 gives examples of commonlyused image planes and patient positions.5,35,37
PULSE SEQUENCES AND IMAGING PARAMETERS
Spin-echo sequences (Fig. 8.5) using short echo time (TE), repetition time (TR) (T1-weighted), and long TE and TR (T2-weighted) provide the necessary information for diagnosis and evaluation of most calf, foot, and ankle disorders (Table 8.1).2,5,29,32,38 Today, T1-weighted, proton density and T2-weighted fast spin-echo (FSE) sequences with or without fat suppression have replaced conventional spin-echo sequences in most situations. We generally perform at least two pulse sequences in at least two image planes (Figs. 8.5,8.6,8.7,8.8,8.9,8.10,8.11). For example, when evaluating the ankle, T2-weighted axial images along with T1- and T2-weighted sagittal images are usually adequate to identify and characterize pathology. Short TI inversion recovery (STIR) or T2* gradient-echo (GRE) sequences can be used in place of FSE T2-weighted images. We also add coronal dual echo steady state (DESS) images to evaluate the articular cartilage (Fig. 8.5F) (Table 8.1). Similarly, two image planes are useful for detection and demonstrating the extent of pathology in the foot. In certain cases, special oblique images are necessary to evaluate the tendons, ligaments, and small osseous structures of the foot and ankle.5,20,32,35,37
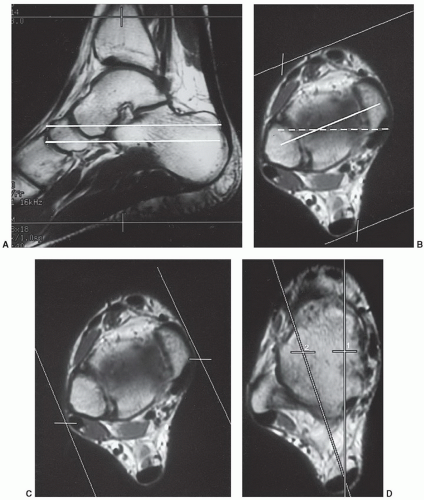
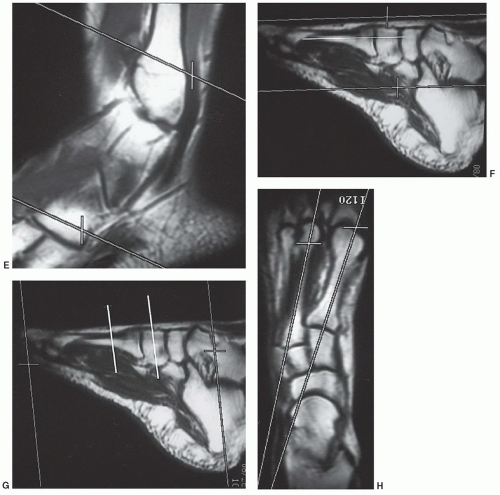
Figure 8.4 Image planes for foot and ankle MRI. A: Foot positioned for axial images of the ankles; upper and lower lines mark the area of coverage. Note the Achilles tendon and neutral position of the foot. With axial images, the tarsal bones (white lines) are sectioned out of anatomic alignment. B: Image planes obliqued to obtain true coronal images through the ankle mortise. The white line indicates planes of sections through the mortise. A conventional coronal plane (dotted line) would cut obliquely through the joint and anatomy. C: Oblique sagittal image planes to improve anatomic display of the osseous structures in the ankle. D: Conventional sagittal image plane (1) and obliqued sagittal plane (2) to improve evaluation of the Achilles tendon. E: Obliqued axial image planes to improve evaluation of the peroneal tendon. F: Scout sagittal image of the mid and forefoot, with the area scanned for images in the planes of the distal tarsal bones and metatarsals (white line indicates the image plane). G: Scout sagittal image for imaging perpendicular to the distal tarsal row and metatarsals (white lines indicate image sections). H: Axial forefoot scout demonstrating oblique planes (lines) for sagittal images of the first and second metatarsals.
Figure 8.4 (continued)
Additional parameters include a small field of view (FOV) (8 to 16 cm), 256 × 256 or 256 × 192 matrix, one acquisition, and 2- to 4-mm slice thickness with 0.2- to 0.5-mm interslice gaps appear to be most useful for defining complex foot and ankle anatomy when surface coils are used. Thicker sections may be used for screening the soft tissues in the leg (Table 8.1). We initially obtain a scout view in the plane best suited to select our initial examining sequences. The sagittal or axial plane is most often used for the scout view for the foot and ankle. A coronal scout is most often used for establishing sequences for the calf. The matrix can be reduced to 256 × 128, which allows the scout image to be obtained in approximately 26 seconds using short TE/TR sequences (see Chapter 3 and Table 8.1). Most examinations of the calf or foot and ankle can be performed with imaging times of less than 30 minutes.5,20,39,40
Three-dimensional GRE sequences are useful for reformatting in different image planes and for evaluation of bony trabeculae.5,27 Intravenous gadolinium is frequently added to the examination, especially in patients with suspected infection (Fig. 8.6), inflammatory arthropathies, or neoplasm. Intravenous gadolinium does provide an arthrographic effect by 15 to 30 minutes after injection.41 We do not commonly perform MR arthrography, tenography, or bursography in the foot and ankle.42
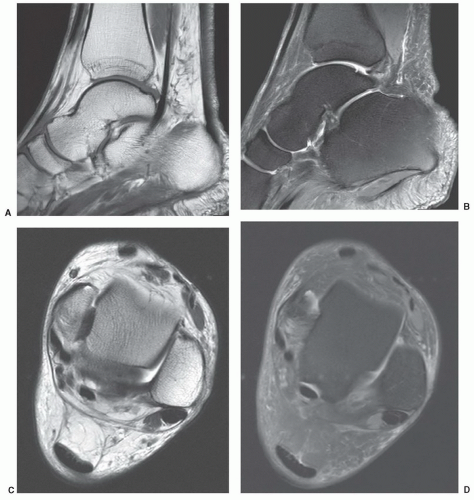
Figure 8.5 3.0 T images of the ankle using screening pulse sequences. Sagittal turbo spin-echo T1-weighted image (700/19, ET 2) (A) and fat suppressed turbo spin-echo proton density weighted (3000/28, ET 8) (B) images. Axial turbo spin-echo T2-weighted image without fat suppression (5160/81, ET 14) (C) and turbo spin-echo proton density weighted image with fat suppression (2000/32, ET 8) (D). Coronal DESS images (9.24/4.05, ET 1) (E) and (13.4/4.85, ET 2) (F). Note the marrow detail in E and excellent cartilage detail in F.
MR angiography has improved using new techniques with contrast enhancement. Distal digital arteries can be identified using contrast-enhanced three-dimensional angiography.43 Therefore, this approach is of value in patients with diabetes mellitus or peripheral vascular disease.21,43
The above general approaches can be applied to adults and children. Children younger than 5 years of age may require sedation. For this purpose, chloral hydrate is most often employed5,44,45 (see Chapter 3).
Figure 8.5 (continued)
Selected techniques and pulse sequences will be defined more completely later as they apply to specific clinical indications.
ANATOMY
MRI provides more diagnostic information than conventional techniques owing to improved tissue contrast and the ability to obtain multiple image planes. Therefore, a thorough knowledge of skeletal and soft tissue anatomy is even more essential than with other imaging techniques. Mastering the anatomy and biomechanics of the calf, foot, and ankle is important for evaluating MR images (Figs. 8.7,8.8,8.9,8.10,8.11).
SKELETAL AND ARTICULAR ANATOMY
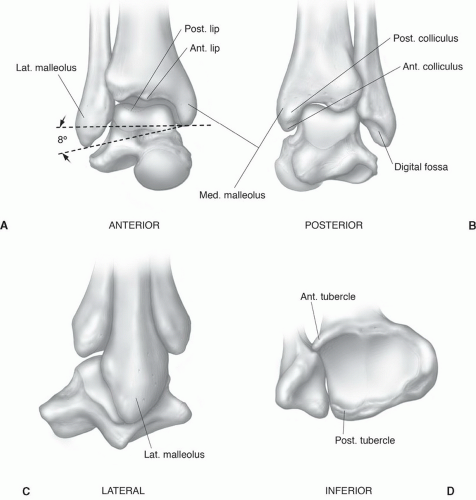
The ankle is composed of three osseous structures: The tibia, fibula, and talus (Fig. 8.12).46,47,48,49 The triangular diaphysis of the tibia, with its three surfaces (anterior, medial, and posterior), expands at the metaphysis forming the medial malleolus and the articular surface for the talus (Fig. 8.8). The articular surfaces are covered by hyaline cartilage except in the most posterior aspect of the tibia. The anterior tibia is typically smooth except for a rough anterior margin for the attachment of the anterior capsule. Posteriorly the tibia contains grooves for the flexor hallucis longus, flexor digitorum longus, and tibialis posterior tendons (Fig. 8.7).24,47,50 Posterolaterally the tibia articulates with the fibula and is supported by the interosseous membrane and anterior and posterior distal tibiofibular ligaments (Fig. 8.7).5,47,48,49,50,51,52
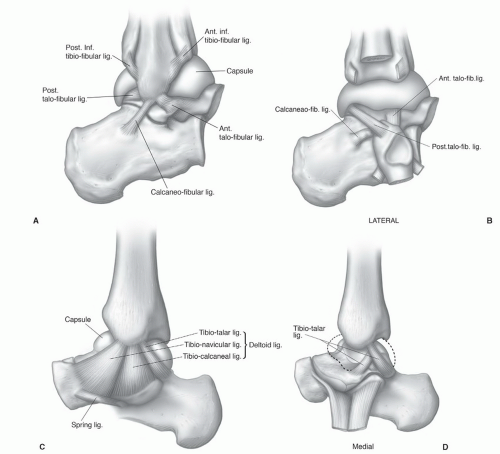
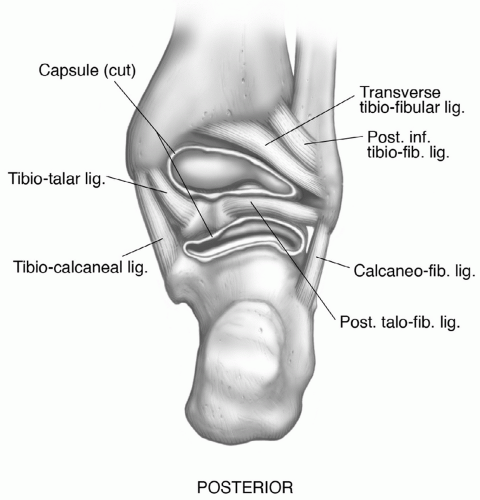
Supporting structures of the ankle are sometimes difficult to demonstrate with MRI, even when using off-axis oblique planes (Figs. 8.7,8.8,8.9,8.10,8.11).5,37,53 These supporting structures include the joint capsule, medial and lateral ligaments, and interosseous ligament (Fig. 8.13). In addition, 13 tendons cross the ankle, and there are 4 retinacula about the ankle (Figs. 8.7, see also Figs. 8.23 and 8.25). The interosseous ligament or membrane has obliquely oriented fibers and joins the tibia and fibula to its distal extent, which is just above the ankle joint. Projecting up between the distal tibia and fibula and below the interosseous ligaments, the syndesmotic recess is seen as an area of high signal intensity extending from the joint proper on MR images (Figs. 8.7 and 8.8). Just above the tibiotalar joint, the distal anterior and distal posterior tibiofibular ligaments provide additional support as they attach to the tibia and fibula anteriorly and posteriorly (Fig. 8.13). Just anterior to the posterior tibiofibular ligament is the transverse ligament, which makes up the fourth ligament of this syndesmotic group. This ligament lies anterior to the posterior tibiofibular ligament and extends from the lateral malleolus to the posterior articular margin of the tibia just lateral to the medial malleolus (Fig. 8.14).5,24,29,47,49,50,54
Medially, the deltoid ligament is a strong triangular group of fibrous tissue with its apex at the medial malleolus. As it passes caudally, the ligament fans out in a triangular fashion and divides into superficial and deep fibers. Distal insertion of this ligament is the navicular tuberosity anteriorly. The remaining fibers insert in the sustentaculum tali and talus (Fig. 8.13).38,50 The spring ligament (plantar calcaneonavicular ligament) (Fig. 8.13C) is important for stabilizing the longitudinal arch. This complex structure is difficult to evaluate on MR images due to its complex multidirectional fibers. The spring ligament is important to evaluate in patients with posterior tibial dysfunction and will be discussed more completely later.29,47,49,50
Table 8.1 MR Examinations of the Calf, Foot, and Ankle
FS, fat suppression; FSE, fast spin-echo; PD, proton density; STIR, short TI inversion recovery; DESS, dual echo steady state.
a The body, extremity, or head coil can be used depending on the area to be studied. b Image plane perpendicular to the sagittal to obtain true cross-sections of the forefoot.
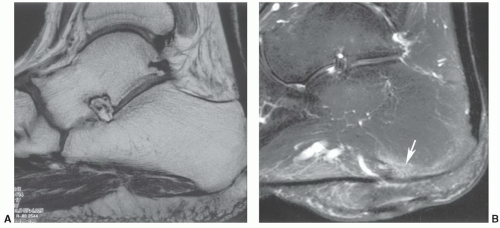
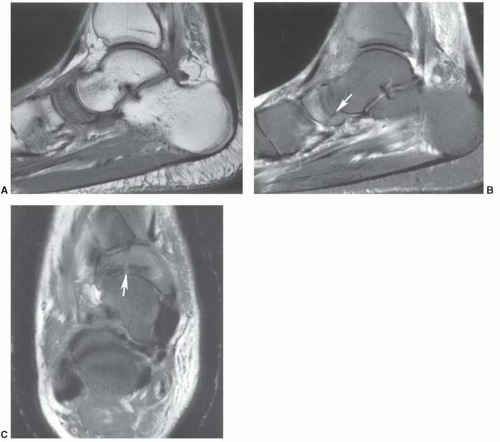
Figure 8.6 Pre- and postadministration of gadolinium intravenously. T1-weighted pre- (A) and post-gadolinium fat-suppressed T1-weighted image (B) demonstrating calcaneal enhancement due to osteomyelitis (arrow).
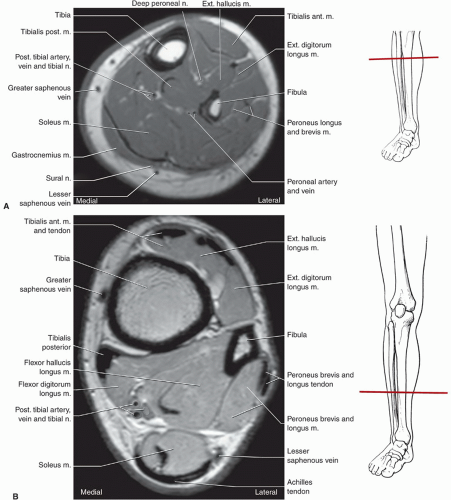
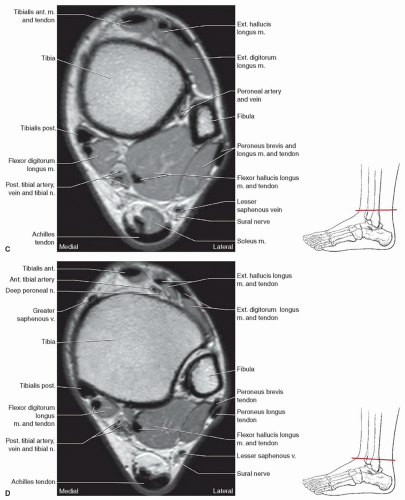
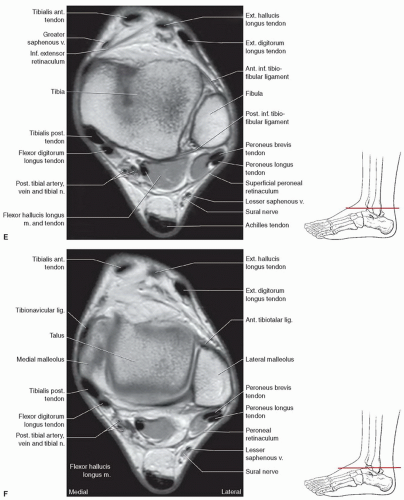
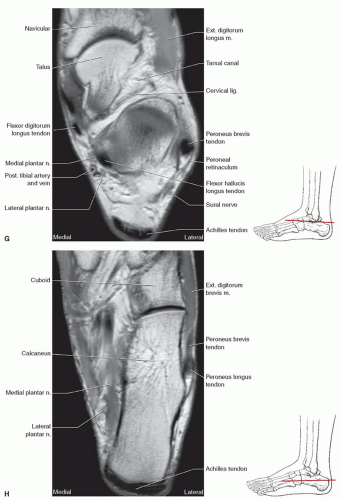
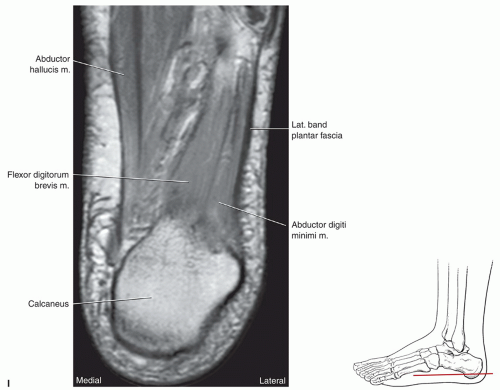
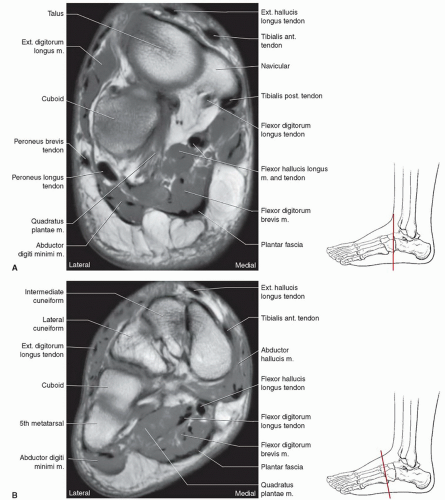
Figure 8.7 Axial T1-weighted images of the calf and ankle with level of section demonstrated. A: Axial image through the upper calf. B: Axial image through the lower calf. C: Axial image through the upper ankle. D: Axial image through the upper syndesmosis. E: Axial image through the lower syndesmosis. F: Axial image through the malleoli and talus. G: Axial image through the tarsal canal. H: Axial image through the calcaneocuboid articulation. I: Axial image through the plantar aspect of the foot.
Figure 8.7 (continued)
Figure 8.7 (continued)
Figure 8.7 (continued)
There are three ligaments in the lateral complex (Fig. 8.13).50,55,56 The anterior talofibular ligament is the weakest and most frequently injured. It passes anteriorly from the fibula to insert on the anterior to the lateral talar articular facet. The posterior ligament is much stronger than the anterior and has a nearly transverse or horizontal course from the posterior aspect of the lateral malleolus to the posterior talar tubercle. The longest of the three ligaments is the calcaneofibular ligament, which takes a nearly vertical course from the lateral malleolus to the lateral surface of the calcaneus. The peroneal tendons lie just superficial to the calcaneofibular ligament. Demonstration of all three of these ligaments is difficult on typical orthogonal MR images due to partial volume effects and the variations in the obliquity of these ligaments (Figs. 8.7, 8.8, 8.9, 8.10, and 8.13).29,47,49,50,55 Oblique image planes, reformatted thin-section three-dimensional images, or MR arthrography are most useful for evaluating these structures.
Figure 8.7 (continued)
Muhle et al.29 found an inhomogeneous appearance of the medial collateral and the posterior talofibular ligaments on T1-weighted images that correlated with areas of fatty tissue located between ligamentous fibers.
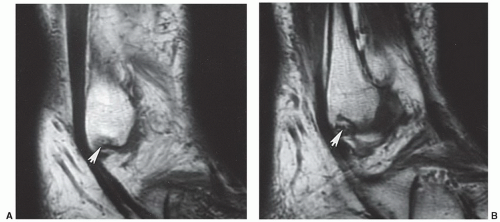
The foot is often divided into three segments: The hindfoot, comprised of the talus and calcaneus; the midfoot, the remaining five tarsal bones; and the forefoot, comprised of the metatarsals and phalanges.47,50 The talus is the second largest of the tarsal bones and articulates with the tibia superiorly, medial and lateral malleolus and calcaneus inferiorly. The head of the talus articulates with the navicular (Figs. 8.7, 8.8, 8.9, 8.10). There are three subtalar articular facets. The anterior and posterior facets articulate with similarly named calcaneal facets. The middle facet is just posterior to the anterior calcaneal articular facet and articulates with the sustentaculum tali (Figs. 8.7 and 8.10).49,50,54,57 The tarsal canal or sinus lies between the middle and anterior facets. The interosseous talocalcaneal ligament lies within this canal and is usually easily seen on sagittal MR images (Fig. 8.10). The tarsal canal has an oblique course between the talus and calcaneus measuring 10 to 15 mm in height and 5 mm in width, with a length of 15 to 20 mm. This appearance on sagittal MR images can be confusing and gives the impression of synovitis with erosive changes in the talus (Fig. 8.10).22,47,49,57,58 In addition to the three superior facets, the calcaneus articulates anteriorly with the cuboid. There are two main ligaments that directly support the talocalcaneal joint. These are the interosseous talocalcaneal ligament, located in the tarsal canal or sinus tarsi, and the smaller lateral talocalcaneal ligaments. Ligaments of the ankle and adjacent tendons provide additional stabilization.24,47,49,50,57,58
Figure 8.8 Coronal DESS images of the ankle and hindfoot from posterior to anterior with level of section demonstrated. A: Coronal image through the calcaneus. B: Coronal image through the lateral malleolus. C: Coronal image through the ankle mortise and sustentaculum. D: Coronal image through the tarsal sinus.
Figure 8.8 (continued)
Figure 8.9 Coronal T1-weighted images through the mid and forefoot with level of section demonstrated. A: Coronal image through the tarsal bones. B: Coronal image through the cuneiforms. C: Coronal image through the proximal metatarsals. D: Coronal image through the mid metatarsal region. E: Coronal image through the first metatarsal sesamoids.
Figure 8.9 (continued)
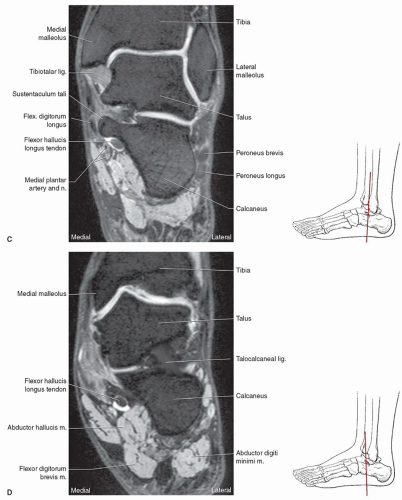
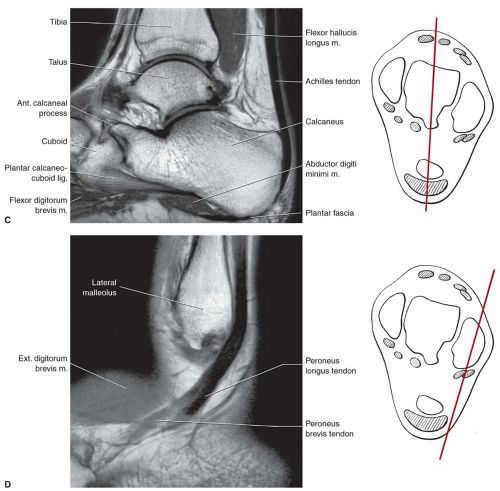
Figure 8.10 Sagittal T1-weighted images of the ankle with level of section demonstrated. A: Sagittal image through the tibialis posterior. B: Sagittal image through the sustentacular level. C: Sagittal image through the talus. D: Sagittal image through the peroneal tendons.
Figure 8.10 (continued)
The remaining tarsal bones (cuboid, navicular, and three cuneiforms) make up the midfoot.49,50,54 The cuboid articulates with the calcaneus proximally and distally with the fourth and fifth metatarsals (Figs. 8.9 and 8.10). The lateral aspect of the cuboid contains a groove for the peroneus longus tendon (Fig. 8.7). The medial surface of the cuboid has an articular facet for the lateral cuneiform. Medially, the navicular articulates with talus proximally and anteriorly with the cuneiforms and occasionally the lateral aspect of the cuboid. An additional ligamentous structure, the spring ligament, extends from the calcaneus to the navicular tuberosity (Figs. 8.10 and 8.13). There are other interosseous ligaments both on the dorsal and plantar surfaces of the tarsal bones.47,49,50
There are three cuneiforms located distal to the navicular and medial to the cuboid. The medial cuneiform is the largest and articulates with the navicular proximally and the intermediate cuneiform laterally. Distally, it articulates with the first and second metatarsals. Lying between medial and lateral cuneiform is the intermediate cuneiform that is the smallest of the three tarsal bones. It articulates with the latter and the navicular proximally and second metatarsal distally. The lateral cuneiform lies between the intermediate cuneiform and the cuboid. It articulates with both of these osseous structures plus the navicular proximally and the second through fourth metatarsals.49,50
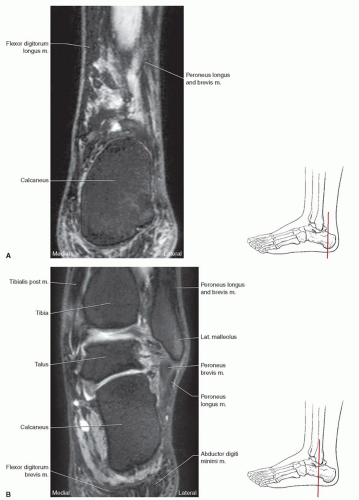
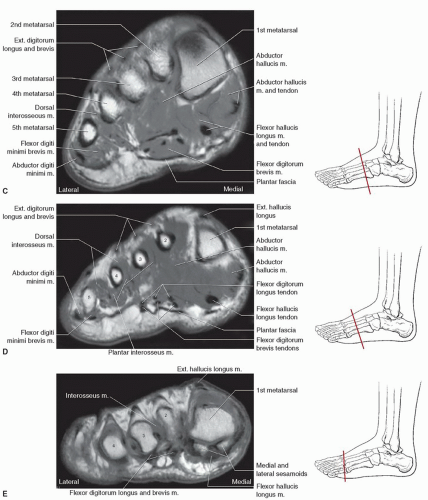
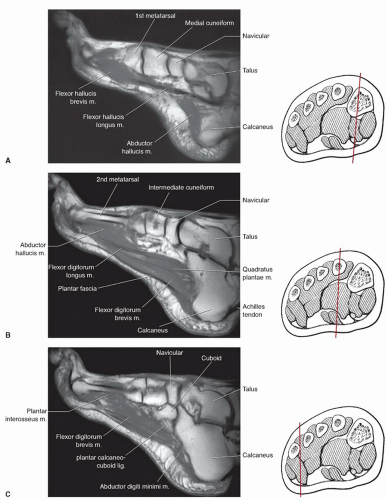
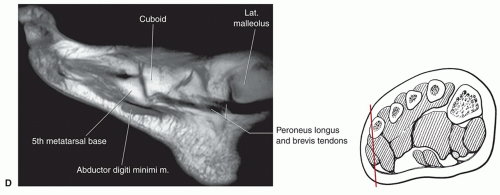
Figure 8.11 Sagittal images of the foot with level of section demonstrated. A: Sagittal image through the medial cuneiform and first metatarsal. B: Sagittal image through the second metatarsal. C: Sagittal image through the calcaneocuboid articulation. D: Sagittal image through the fifth metatarsal base.
Figure 8.11 (continued)
Figure 8.12 Illustrations of the ankle seen from the anterior (A), posterior (B), lateral (C), and infratibial (D) surfaces. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
Figure 8.13 Illustrations of the capsule (A), lateral (B), and medial (C and D) ligaments of the ankle. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
There are five metatarsals that articulate with the tarsal bones. Each has three phalanges with the exception of the great toe, which typically has two. The dorsal, plantar, and interosseous ligaments support the tarsometatarsal joints and bases of the metatarsals. Distally, the transverse metatarsal ligament connects the heads of all five metatarsals. The metatarsophalangeal (MTP) joints are supported by collateral ligaments and plantar ligaments. Dorsally, the extensor tendons replace the usual dorsal ligaments seen in the midfoot (Figs. 8.67 and 8.9).24,49,50,54,59,60
Marrow patterns vary with age on MR images. Pal et al.61 found that 63% of symptomatic and 57% of asymptomatic children had marrow patterns in the feet that varied from multiple distinct foci to confluent areas of low T1-weighted signal and high signal intensity on T2-weighted and STIR images. Heterogeneous bone marrow in the feet in the immature skeleton can be a normal finding.61
Figure 8.14 Illustrations of ligaments of the ankle seen posteriorly. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
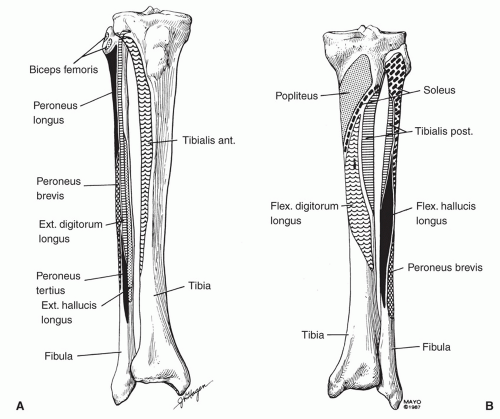
Figure 8.15 Anterior (A) and posterior (B) illustrations of the tibia and fibula demonstrating origins of muscles that insert on or affect the foot and ankle. (From Berquist TH. Radiology of the Foot and Ankle. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2000.)
SOFT TISSUE ANATOMY
The lower extremity musculature develops from mesodermal tissues of the lower limb bud.47,49,50,54 Functional muscle groups are organized in fascial compartments. To simplify the muscular anatomy of the foot and ankle, we will discuss compartments or functional groups of muscles, including their origins, insertions, and actions. Normal variants will also be discussed.
Themuscles of the leg can be dividedintoanterior, posterior, and lateral compartments. One of these muscles crosses only the knee, and the other two cross the knee and ankle. The majority arise in the leg and act on both the foot and ankle (Fig. 8.15).5,20,47,49,50,54,62,63
POSTERIOR MUSCULATURE
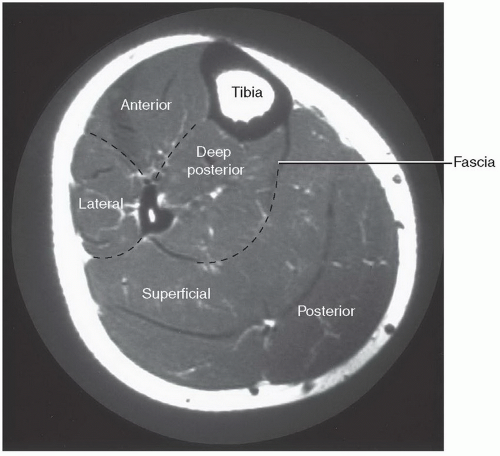
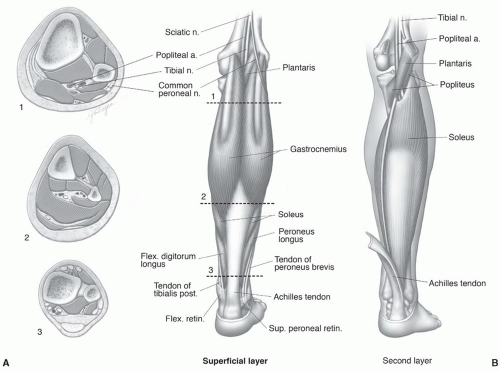
The superficial and deep muscles of the calf are divided into compartments by the crural fascia (Fig. 8.16).47,50 The superficial muscle group includes the gastrocnemius, soleus, and plantaris (Fig. 8.17). The gastrocnemius has two heads arising from the medial and lateral femoral condyles (Fig. 8.18). The two heads unite to form the bulk of the muscle in the upper calf (Fig. 8.7A). At about the midpoint of the calf, the muscle ends in a wide, flat tendon. The soleus inserts into the anterior aspect of the gastrocnemius tendon. Below this level, the tendon narrows in transverse diameter and thickens forming the Achilles tendon (tendo calcaneus), which inserts on the posterior calcaneus (Figs. 8.7, 8.10, and 8.17). The gastrocnemius plantar flexes the foot and also assists in knee flexion during non-weight bearing. Innervation is by the tibial nerve and the vascular supply primarily derived from the posterior tibial artery (Table 8.2).47,49,50
Figure 8.16 Axial MR image of the calf demonstrating the compartments with crural fascia separating the deep and superficial posterior muscle groups.
Figure 8.17 Illustration of the posterior leg. A: Illustration of the superficial musculature with cross-sections at levels 1, 2, 3. B: Illustration of the soleus, plantaris, and upper vascular relationships. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
The soleus muscle lies deep to the gastrocnemius (Figs. 8.7 and 8.17) and also has two heads, one arising from the posterior superior fibula and the second from the popliteal line and posteromedial surface of the proximal tibia (Fig. 8.15). The popliteal vessels and tibial nerve pass deep to the body of the soleus. The soleus inserts in the anterior aspect of the gastrocnemius tendon, forming the thicker Achilles tendon.5,47,50
The soleus muscle (Fig. 8.18) has no effect on the knee, but serves as a plantar flexor of the foot. Innervation is via the tibial nerve, with vascular supply from the posterior tibial artery (Table 8.2).
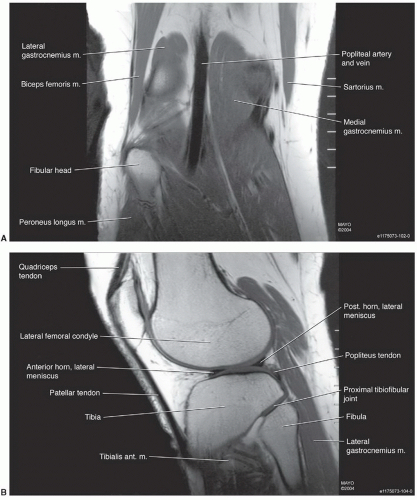
Figure 8.18 Coronal (A) and sagittal (B) T1-weighted images of the knee, demonstrating the origins of the gastrocnemius muscles.
The plantaris is the third muscle included in the superficial compartment (Fig. 8.17). This small muscle takes its origin from the lateral epicondyle of the femur and the oblique popliteal ligament. The belly of the muscle is only several inches long and passes between the gastrocnemius and soleus in an oblique direction (Fig. 8.17). The long, thin tendon passes distally along the medial margin of the Achilles to insert in the calcaneus, Achilles, or flexor retinaculum. Occasionally the muscle is double and may be totally absent.49 The plantaris functions as a minor flexor of the knee and plantar flexor of the foot. Innervation and blood supply are from the tibial nerve and posterior tibial artery (Table 8.2).47,49
Table 8.2 Muscles of the Leg, Foot and Ankle
Location
Muscle
Origin
Insertion
Action
Innervation (Segment)
Blood Supply
Calf
Superficial compartment
Gastrocnemius
Femoral condyles
Posterior calcaneus
Flexor of foot and knee
Tibial nerve (S1,S2)
Posterior tibial artery
Soleus
Upper tibia and fibula
Gastrocnemius tendon
Plantar flexor of foot
Tibial nerve (S1,S2)
Posterior tibial artery
Plantaris
Lateral femoral condyle and oblique popliteal ligament
Posteromedial calcaneus
Plantar flexes foot, flexes leg
Tibial nerve (L4-S1)
Posterior tibial artery
Deep compartment
Popliteus
Lateral femur and capsule of knee
Flexion and medial rotation of leg
Tibial nerve (L5,S1)
Posterior tibial artery
Flexor hallucis longus
Posterior mid fibula
Distal phalanx great toe
Flexor great toe and ankle
Tibial nerve (L5-S2)
Posterior tibial artery
Flexor digitorum longus
Posterior tibia
Distal phalanges second to fifth toes
Flexes toes and foot and supinates ankle
Tibial nerve (L5,S1)
Posterior tibial artery
Tibialis posterior
Posterior tibia, fibula, and interosseous membrane
Navicular, cuneiform, calcaneus, second to fourth metatarsals
Adduction of forefoot, hindfoot, inversion, plantar flexion
Tibial nerve (L5,S1)
Posterior tibial artery
Lateral compartment
Peroneus longus
Lateral fibula
First metatarsal and medial cuneiform
Evertor and weak plantar flexors
Superficial and deep peroneal nerve (L4-S1)
Peroneal artery
Peroneus brevis
Lateral fibula
Base fifth metatarsal
Superficial peroneal nerve (L4-S1)
Peroneal artery
Anterior compartment
Extensor digitorum longus
Upper tibia, fibula, and interosseous membrane
Lateral four toes
Dorsiflexes toes, everts foot
Deep peroneal nerve (L4-S1)
Anterior tibial artery
Peroneus tertius
Distal fibula and interosseous membrane
Base fifth metatarsal
Dorsiflexes and everts foot
Deep peroneal nerve (L4-S1)
Anterior tibial artery
Extensor hallucis longus
Distal fibula and interosseous membrane
Distal phalanx great toe
Extends great toe, weak invertor and dorsiflexion of foot
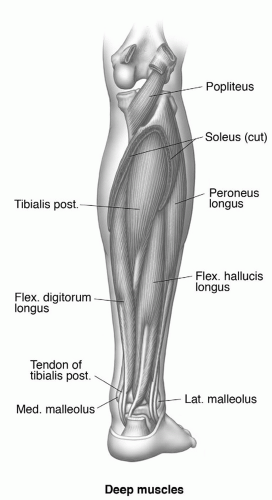
The deep compartment of the calf contains the popliteus, tibialis posterior, flexor hallucis longus, and flexor digitorum longus muscles (Figs. 8.7,8.8,8.9,8.10,8.11, and 8.19).47,49,50
The popliteus is a small triangular muscle forming a portion of the floor of the popliteal fossa (Fig. 8.19). Its origin is from the lateral femoral condyle, the arcuate popliteal ligament, and capsule of the knee. The insertion is the posterior surface of the upper tibia above the origin of the soleus (Fig. 8.19). The popliteus acts on the knee and leg as a flexor and medial rotator. Neurovascular supply is by the tibial nerve and posterior tibial artery (Table 8.2).47,49,50,62
The flexor hallucis longus is the most lateral of the three remaining deep muscles of the leg (flexor hallucis longus, flexor digitorum longus, and tibialis posterior) (Figs. 8.7 and 8.19). It arises from the lateral aspect of the middle half of the posterior fibula (Fig. 8.15).49,50,62 Its tendon begins above the malleoli of the ankle and courses medially behind the ankle deep to the flexor retinaculum (Fig. 8.19). The tendon is posterior to the tendons of the tibialis posterior and flexor digitorum longus behind the medial malleolus (Figs. 8.7 and 8.19). The posterior aspect of the talus contains an oblique groove (Fig. 8.20) for the flexor hallucis longus tendon.24,47 The tendon passes along the plantar aspect of the foot to insert in the distal phalanx of the great toe (Figs. 8.7 and see Fig. 8.29). The flexor hallucis longus is a flexor of the great toe and assists in ankle flexion. The muscle is innervated by the tibial nerve and receives its blood supply from the posterior tibial artery (Table 8.2).47,49,62
Figure 8.19 Illustration of the deep muscles of the calf. (From Berquist TH. Radiology of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
The flexor digitorum longus lies medially in the deep compartment of the calf (Fig. 8.7). It arises from the upper half of the posteromedial aspect of the tibia (Fig. 8.15). Along its caudad course it passes posterior to the tibialis posterior so that at the ankle it lies between the flexor hallucis longus and tibialis posterior (Fig. 8.7). The tendon passes through the flexor retinaculum, posterior to the medial malleolus, and then divides into four slips that insert in the distal phalanges of the lateral four digits (Figs. 8.19 and 8.29). On the plantar aspect of the foot, these four tendon slips are associated with the lumbrical muscles and pass through the divided slips of the flexor digitorum brevis prior to inserting on the distal phalanges.5,49,62
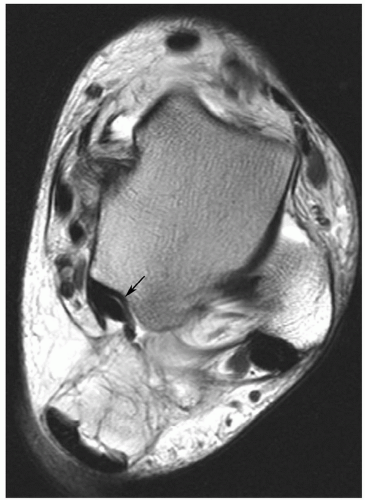
Figure 8.20 3.0 proton density weighted axial image demonstrating the talar groove for the flexor hallucis longus tendon (arrow).
The flexor digitorum longus flexes the lateral four toes and also plantar flexes the foot and supinates the ankle. The muscle is innervated by branches of the tibial nerve and receives its vascular supply from posterior tibial artery branch (Table 8.2).24,47
The tibialis posterior is the deepest and most centrally located muscle in the deep posterior compartment (Figs. 8.7 and 8.19). It arises from the upper posterior aspects of the tibia and fibula and the interosseous membrane (Fig. 8.15). Thus, it is positioned between the flexor hallucis longus and flexor digitorum longus. Therefore, it is the most anterior of the three tendons as it passes behind the medial malleolus (Fig. 8.7). The tendon flares to insert in the navicular, tarsal bones, and bases of the two to three metatarsals (Figs. 8.7, 8.21, and 8.31).49,50,52
The tibialis posterior aids in adduction, inversion, and plantar flexion of the foot. The muscle is innervated by branches of the tibial nerve and receives its blood supply from the posterior tibial artery (Table 8.2).47Table 8.2 summarizes the muscles of the calf and their functions.
NEUROVASCULAR ANATOMY OF THE CALF
The tibial nerve is a continuation of the sciatic nerve at the level of the popliteal fossa. As the nerve passes inferiorly, it enters the calf between the heads of the gastrocnemius muscle, passing deep to the soleus to lie between the soleus and tibialis posterior in the deep compartment (Figs. 8.7 and 8.22).47,49 The tibial nerve sends branches to all of the superficial and deep muscles of the calf (Table 8.2). At the ankle level, the nerve generally lies between the flexor hallucis longus and flexor digitorum longus tendons (Fig. 8.7). Distal to the flexor retinaculum, it divides, forming the medial and lateral plantar nerves.49,50
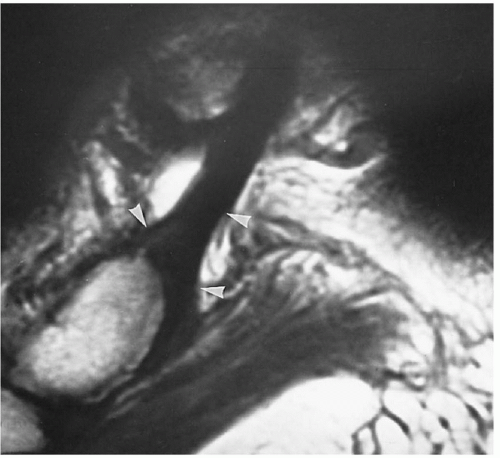
Figure 8.21 Sagittal T1-weighted image demonstrating the normal flare or widening (arrowheads) of the tibialis posterior tendon as it inserts onto the navicular.
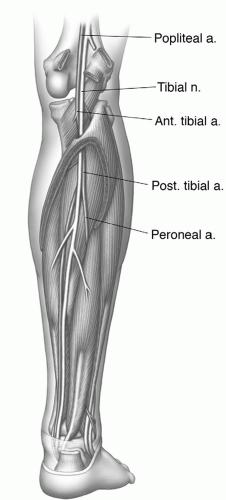
The popliteal artery is a direct continuation of the superficial femoral artery as it passes through the adductor canal (Fig. 8.22). It divides into anterior and posterior tibial branches at the level of the popliteus muscle. The anterior tibial artery enters the anterolateral leg above the upper margin of the interosseous membrane, whereas the posterior tibial artery joins the tibial nerve in the deep compartment of the calf (see Figs. 8.22 and 8.26). In the leg, it provides muscular branches to all of the calf muscles and a nutrient artery to the tibia. Its largest branch, the peroneal artery, arises high in the leg and passes deep to the flexor hallucis longus near the interosseous membrane and fibula (Figs. 8.7 and 8.22). At the ankle level, it forms anastomotic branches with the posterior tibial artery and perforates the interosseous membrane to supply the dorsal aspect of the foot. Generally, paired veins accompany the arteries. These veins are more variable and enter the popliteal vein superiorly.46,49,50
ANTEROLATERAL MUSCULATURE
The peroneus longus and brevis are the two muscles of the lateral compartment. Both arise from the superior lateral surface of the fibula. The origin of the peroneus longus is more superior, with the muscle passing superficial to the peroneus brevis (Fig. 8.15). The muscles progress caudad in the lateral compartment, with their tendons entering a common tendon sheath above the ankle (Figs. 8.7, 8.10, and 8.23).The tendons pass posterior to the lateral malleolus and deep to the superior and inferior peroneal retinacula. The tendons diverge on the lateral surface of the foot (Fig. 8.24) with the peroneus brevis inserting on the base of the fifth metatarsal. The peroneus longus takes an inferior course passing under the lateral aspect of the foot where it inserts on the base of the first metatarsal and medial cuneiform (Fig. 8.31).24,47,49
Figure 8.22 Illustration of the major neurovascular structures in the calf. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
These muscles serve as evertors of the foot and assist in plantar flexion. Innervation is from the superficial peroneal nerve, with branches of the common or deep peroneal nerve supplying a portion of the peroneus longus. Vascular supply is via the peroneal artery (Table 8.2).50
ANTERIOR COMPARTMENT MUSCULATURE
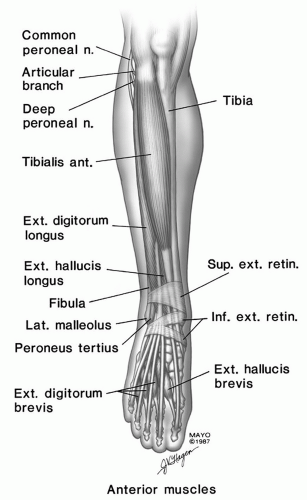
There are four muscles in the anterior compartment. These include the extensor digitorum longus, peroneus tertius, extensor hallucis longus, and tibialis anterior (Figs 8.7 and 8.25) (Table 8.2).
The extensor digitorum longus is the most lateral muscle in the anterior compartment (Figs. 8.6 and 8.25). It arises from the lateral tibial condyle, anterior fibula, and interosseous membrane (Fig. 8.15). The tendon passes deep to the superior and inferior extensor retinaculae prior to dividing into four slips that insert and the dorsal aspects of the four lateral toes (Fig. 8.25). The insertions are divided such that portions insert in the middle and distal phalanges.56,64 The extensor digitorum longus dorsiflexes the toes and also assists in eversion of the foot. It is innervated by the deep peroneal nerve and receives its vascular supply from the anterior tibial artery (Table 8.2). Variations in its origin and distal insertions are not uncommon, but these rarely cause confusion on MR images.47,49
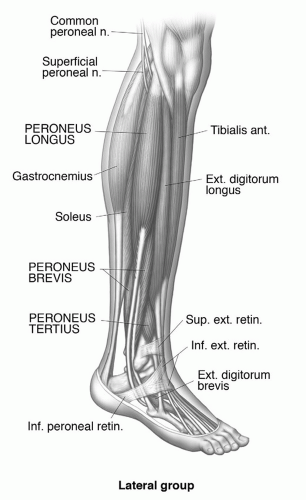
Figure 8.23 Illustration of the lateral muscle group of the leg. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
The peroneus tertius is closely associated with the extensor digitorum longus, and may be considered a portion of the latter.47 It arises from the distal anterior fibula, interosseous membrane, and membrane of the peroneus brevis (Fig. 8.15). Its tendon passes deep to the extensor retinaculae to insert on the dorsal aspect of the base of the fifth metatarsal (Fig. 8.25). Neurovascular supply to the peroneus tertius is via the deep peroneal nerve and anterior tibial artery. This muscle varies in size and may be absent (Table 8.2).24,50
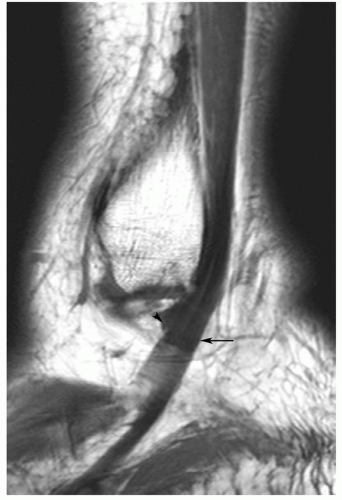
Figure 8.24 Sagittal proton density weighted image demonstrating the peroneus brevis (arrowhead) and longus (arrow) passing inferior to the lateral malleolus.
The tibialis anterior muscle arises from the lateral tibia surface, deep fascia, and interosseous membrane (Fig. 8.15). It passes inferiorly, becoming tendonous in the lower leg; it is the most medial tendon as it passes deep to the extensor retinaculae (Fig. 8.7). It passes along the medial foot to insert in the medial cuneiform and plantar portion of the first metatarsal (Fig. 8.25).49,50 This muscle is a strong dorsiflexor and inverter of the foot. Neurovascular supply is via the deep peroneal nerve and anterior tibial artery (Table 8.2).47
NEUROVASCULAR ANATOMY OF THE ANTEROLATERAL MUSCLES
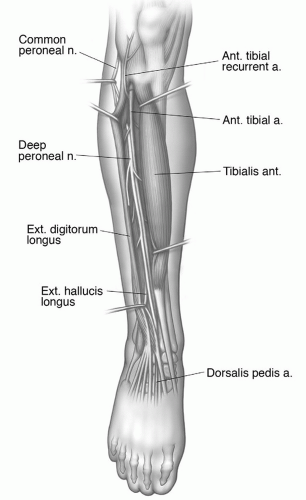
The common peroneal nerve is a branch of the sciatic nerve and courses laterally in the popliteal fossa. It is subcutaneous and relatively unprotected just below the fibular head (Fig. 8.26). Therefore, it is susceptible to direct trauma in this area.5,49 As it descends between the fibula and peroneus longus, it divides into two or three branches. These are the superficial, deep, and articular branches of the peroneal nerve. The superficial peroneal nerve lies between the peroneus longus and brevis and supplies these muscles and the subcutaneous tissues. The deep peroneal nerve courses anteriorly, deep to the peroneus longus, to supply the anterior muscles of the leg (Table 8.2). It joins the anterior tibial artery on the anterior aspect of the interosseous membrane.47,49
Figure 8.25 Illustration of the anterior compartment muscles. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
The anterior tibial artery passes superior to the interosseous membrane in the upper leg and then lies with the deep peroneal nerve along the anterior aspect of the interosseous membrane (Fig. 8.26). It supplies the anterior muscles and continues as the dorsalis pedis artery on the dorsum of the foot (Fig. 8.33).47,49Table 8.2 summarizes the muscles of the leg, their functions, and neurovascular supply.
FOOT MUSCULATURE
The muscles of the foot are considered in layers instead of compartments (Fig. 8.27).47,49,50,65
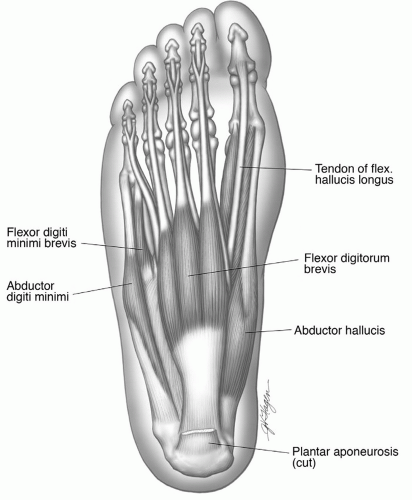
The superficial layer of plantar muscles includes the abductor hallucis, flexor digitorum brevis, and abductor digiti minimi. The abductor hallucis arises from the medial process of tubercle of the calcaneus, the flexor retinaculum, and plantar aponeurosis. Its insertion is the medial side of the flexor surface of the proximal phalanx of the great toe (Figs. 8.7, 8.9, and 8.28).47,49 The medial and lateral plantar vessels and nerves (Fig. 8.7) pass deep to the proximal position of the muscle as they enter the foot. The muscles are supplied by branches of the medial plantar nerve and artery. The abductor hallucis functions weakly as an abductor of the MTP joint of the great toe (Table 8.3).47,49
Figure 8.26 Illustration of the anterior neurovascular anatomy. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
The flexor digitorum brevis is the most central of the superficial plantar muscles (Figs. 8.7, 8.8, and 8.28). It arises from the medial tubercular process of the calcaneus and plantar fascia. Four tendons pass distally and divide into two slips at the level of the proximal phalanx. The tendons of the flexor digitorum longus pass through the divided brevis tendons. The divided tendon slips insert on the middle phalanx.47 The muscle flexes the lateral four toes. The flexor digitorum brevis receives its neurovascular supply from the medial plantar nerve and artery. The lateral plantar nerve and artery pass deep to this muscle. It is not uncommon for the tendon to the fifth toe to be absent (38%) (Table 8.3).47
The abductor digiti minimi is the most lateral muscle in the superficial layer (Figs. 8.7 and 8.28). It arises from the lateral process of the calcaneal tubercle and the distal portion of the medial process. It inserts in the lateral aspect of the base of the proximal phalanx of the fifth toe and serves to flex and abduct the toe at the MTP joint. This muscle receives its neurovascular supply from the lateral plantar nerve and artery (Table 8.3).50
Figure 8.27 Illustration of the muscle layers in the foot. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
Figure 8.28 Illustration of the superficial muscle layers of the foot. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
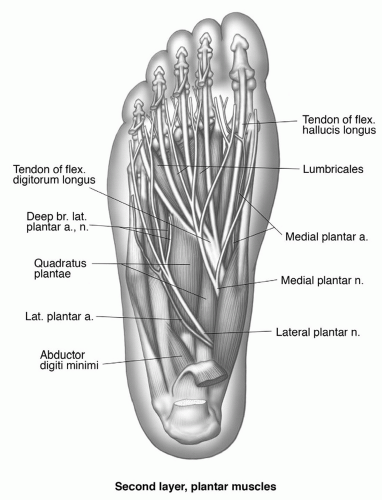
The second layer of the foot is composed of the tendons of the flexor hallucis longus and flexor digitorum longus plus the quadratus plantae and lumbrical muscles (Figs. 8.9 and 8.29).47,49,50
The quadratus plantae has two heads that arise from the medial and lateral plantar aspects of the calcaneal tuberosity. The muscle inserts in the lateral and posterior margin of the flexor digitorum longus just before it divides into its four tendon slips (Figs. 8.7, 8.9, and 8.29).5,47 The muscle assists the flexor digitorum longus in flexing the lateral four toes. The neurovascular supply is provided by the lateral plantar nerve and artery. Occasionally, the lateral head or, in certain cases, the entire muscle may be absent (Table 8.3).47,49
The four lumbrical muscles arise from the flexor digitorum longus tendon. They pass distally to insert on the medial side of MTP joints of the four lateral toes (Fig. 8.29). They act as flexors of the MTP joints. The most medial muscle is innervated by the medial plantar nerve, whereas the lateral plantar nerve supplies the lateral three muscles. Blood supply is via the medial and lateral plantar arteries. Absence of one or more of the lumbricals has been reported. Occasionally, two muscles insert on the fourth and fifth toes (Table 8.3).47
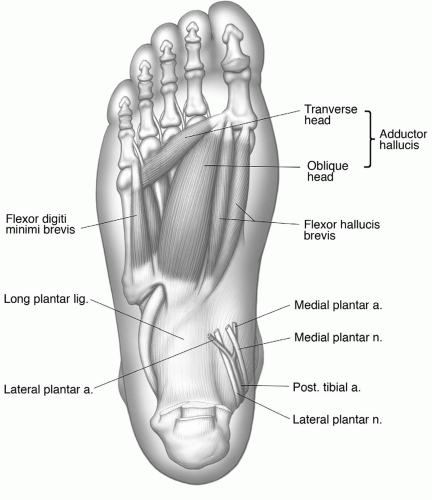
The third layer of plantar muscles includes the flexor hallucis brevis, adductor hallucis, and flexor digiti minimi brevis (see Figs. 8.7 and 8.30). The flexor hallucis brevis has two bellies arising from the plantar aspect of the cuboid and adjacent cuneiform (Fig. 8.30). The tendons insert at the sides of the base of the great toe and the sesamoids. The muscle serves as a flexor of the great toe and is supplied by the medial plantar nerve and artery.5,49,50
Table 8.3 Muscles of the Foot
Location
Muscle
Origin
Insertion
Action
Innervation (Segment)
Blood Supply
Plantar
Superficial first layer
Abductor hallucis
Medial calcaneus, plantar aponeurosis, and flexor retinaculum
Proximal phalanx great toe
Flexor and abductor MTP joint great toe
Medial plantar nerve (L5,S1)
Medial plantar artery
Flexor digitorum brevis
Medial calcaneus plantar fascia
Middle phalanges second to fifth toes
Flexor of toes
Medial plantar nerve (L5,S1)
Medial plantar artery
Abductor digiti minimi
Lateral process calcaneal tubercle
Lateral base proximal phalanx small toe
Abductor and flexor small toe
Lateral plantar nerve (S1,S2)
Lateral plantar artery
Second layer
Quadratus plantae
Medial and lateral calcaneal tuberosity
Flexor digitorum longus tendon
Flexes terminal phalanges two to five Flexes MTP joints
Lateral plantar nerve (S1,S2)
Lateral plantar artery
Lumbricals
Flexor digitorum longus tendon
MTP joints two to five
Medial and lateral plantar nerve (S1,S2)
Medial and lateral plantar arteries
Third layer
Flexor hallucis brevis
Cuboid, cuneiform
Great toe
Flexor great toe
Medial plantar nerve (L5,S1)
Medial and lateral artery
Adductor hallucis
Second to fourth metatarsal bases and third to fifth capsules transverse leg
Great toe
Adductor great toe, maintains transverse arch
Lateral plantar nerve (L5,S1)
Lateral plantar artery
Flexor digiti minimi brevis
Cuboid and fifth metatarsal base
Proximal phalanx fifth toe
Flexes fifth toe
Lateral plantar nerve (S1,S2)
Lateral plantar artery
Fourth layer
Interossei dorsal
Metatarsal bases
Bases of second to fourth proximal phalanges
Abduct toes
Lateral plantar nerve (S1,S2)
Lateral plantar artery
Plantar
Metatarsal bases
Bases of third to fifth proximal phalanges
Abduct toes
Lateral plantar nerve (S1,S2)
Lateral plantar artery
Dorsal
Extensor digitorum brevis
Superior calcaneus, lateral talocalcaneal ligament, extensor retinaculum
The adductor hallucis muscle has oblique and transverse heads (Fig. 8.30). The oblique head arises from the long plantar ligament, and the second through fourth metatarsal bases.49,65 The smaller transverse head arises from the capsules of the third through fifth MTP joints and the deep transverse ligaments. The two heads join lateral to the great toe to insert with the lateral head of the flexor hallucis brevis. The adductor hallucis adducts and flexes the great toe. In addition, it assists in flexion of the proximal phalanx and in maintaining the transverse arch. It is supplied by the lateral plantar arteries and nerves (Table 8.3).47
The flexor digiti minimi brevis arises from the cuboid and base of the fifth metatarsal and inserts in the lateral base of the proximal phalanx of the fifth toe (Fig. 8.30). The muscle serves as a flexor of the small toe and is supplied by branches of the lateral plantar nerve and artery.47,49
Figure 8.29 Illustration of the second muscle layer of the foot with neurovascular structures. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
Figure 8.30 Illustration of the third muscle layer of the foot with plantar nerves. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
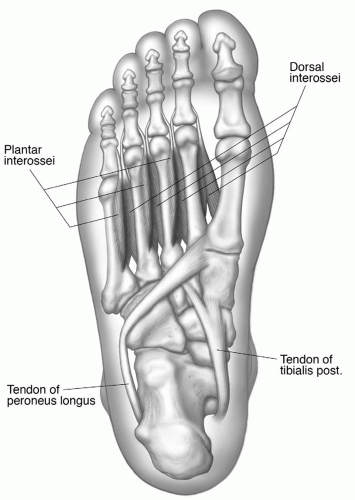
Figure 8.31 Illustration of the deepest (fourth) layer of muscles in the foot, with peroneus longus and posterior tibial tendon insertions. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
The fourth and deepest layer of plantar muscles consists of seven interosseous muscles—three plantar and four dorsal (Figs. 8.9 and 8.31). The four dorsal interossei muscles arise with two heads from the adjacent aspects of the metatarsal bases (Figs. 8.9 and 8.31). The tendons insert into the bases of the proximal phalanges with the two medial bellies inserting on the medial and lateral side of the second and the third and fourth inserting on the lateral sides of the third and fourth proximal phalanges. The three plantar interosseous muscles arise from the bases of the third through fifth metatarsals and insert on the medial sides of the proximal phalanges of the third, fourth, and fifth toes. Thus, the dorsal interossei are abductors and the plantar interossei adductors. All interossei muscles are supplied by branches of the lateral plantar artery and nerve (Table 8.3).47,50
The extensor digitorum brevis (Figs. 8.9 and 8.25) is the dorsal muscle of the foot. This broad, thin muscle arises from the superior calcaneus, lateral talocalcaneal ligament, and extensor retinaculum. It takes a medial oblique course ending in four tendons that insert in the lateral aspect of the proximal phalanx of the great toe and the lateral aspect of the extensor digitorum longus tendons of the second to fourth toes. The muscle extends the great toe and second through fourth toes. Neurovascular supply is provided by the deep peroneal nerve and dorsalis pedis artery.5,47,49 The muscles of the foot are summarized in Table 8.3.
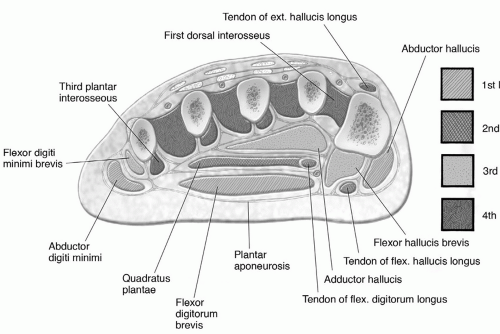
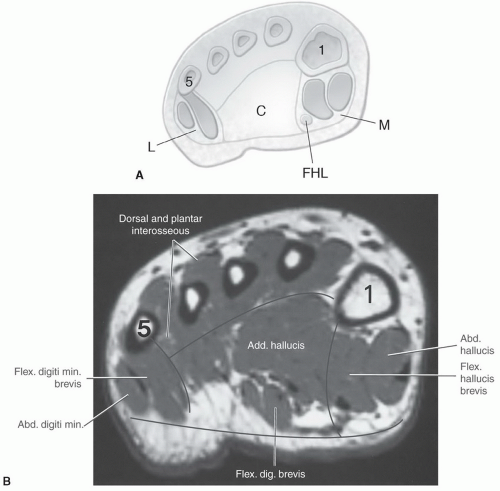
Soft tissue contrast provided by MRI and, to a lesser degree, CT has popularized the compartment concept for evaluating soft tissue infection and neoplasms in the foot.66,67,68,69 Although this concept is controversial, most clinicians consider that the plantar compartments of the foot are divided by intermuscular septa that extend dorsally from the plantar aponeurosis (Fig. 8.32).47,67,69,70,71 The medial septum (Fig. 8.32) courses dorsally from the aponeurosis to attach to the navicular, the medial cuneiform, and the lateral planter aspect of the first metatarsal. The lateral septum (Fig. 8.32) extends from the aponeurosis to the medial aspect of the fifth metatarsal. Thus, the lateral, central or intermediate, and medial compartments are created (Fig. 8.32).49,67,69 The medial compartment contains the abductor hallucis and flexor hallucis and flexor hallucis brevis muscles and the flexor hallucis longus tendon. The lateral compartment contains the flexor digiti minimi brevis and abductor digiti minimi. The central compartment contains three layers described earlier, including the flexor digitorum brevis, the flexor digitorum longus tendon, the quadratus plantae, the lumbrical muscles, and the adductor hallucis.47,67 Spread of infection tends to follow these compartments.
NEUROVASCULAR SUPPLY OF THE FOOT
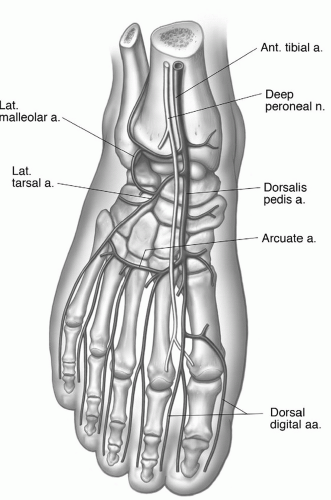
The anterior tibial artery continues over the midanterior aspect of the tibia passing deep to the extensor tendons and retinaculae of the ankle (Fig. 8.33). At the ankle, the anterior tibial artery anastomosis with the perforating branch of the peroneal artery both supply the periarticular structures of the ankle. As the anterior tibial artery emerges from the extensor retinaculum it becomes the more superficial dorsalis pedis artery. After giving off the deep plantar artery, it becomes the first dorsal metatarsal artery. This vessel courses distally, ending in digital branches of the first and second toes. Dorsal branches of the foot include medial and lateral tarsal arteries and the arcuate artery with its dorsal metatarsal branches (Fig. 8.33).47,49
The deep peroneal nerve accompanies the anterior tibial, dorsalis pedis, and first dorsal metatarsal arteries. It supplies the anterior muscles of the foot and leg. The superficial peroneal nerve runs over the anterior aspect of the fibula supplying the peroneal muscles and the lateral aspect of the foot (Fig. 8.32).21,49,50
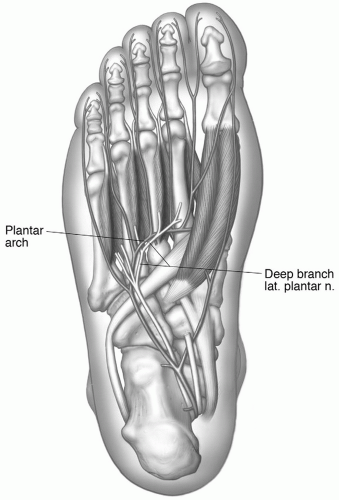
The posterior tibial artery divides into medial and lateral plantar branches deep to the flexor retinaculum. The posterior tibial artery is accompanied by similarly named nerves and veins. The neural branches (medial and lateral plantar nerves) are branches of the tibia nerve (Fig. 8.34).47,49
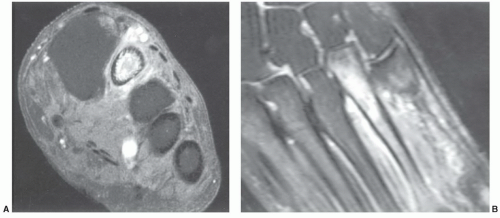
Figure 8.32 A: Axial illustration through the proximal metatarsals demonstrating the lateral, central, and medial compartments. The medial compartment contains the flexor hallucis longus tendon. B: Axial MRI demonstrating the compartments of the foot with muscular anatomy.
The medial plantar artery is the smaller of the two branches of the posterior tibial artery and ends in digital branches to the first toe. The lateral plantar artery is larger and forms an arch at the midfoot level that gives off four metatarsal arteries with their distal digital branches (Fig. 8.34).49 The lateral plantar artery also gives off perforating muscular branches that form anastomoses with the dorsal arteries. Numerous minor variations in the digital arteries have been described.21,47,49
The peroneal artery passes inferior to the lateral malleolus and ends on the calcaneal surface in the lateral calcaneal artery.47,49
Table 8.3 summarizes the neurovascular supply to the muscles of the foot.
PITFALLS AND NORMAL VARIANTS
Misinterpretation of MR images can be related to partial volume effects, flow and other artifacts, failure to review associated radiographs, and normal anatomic variants. Recognition of these nonpathologic conditions is important to prevent misinterpretation of images and unnecessary treatment.5,40,72,73,74,75,76
There are numerous soft tissue variants in the calf, foot, and ankle.38,70,73,74,75 Muscle variations can cause particular confusion when accessing subtle changes on MR images. For example, the gastrocnemius may have only one head, typically the medial head.47,49 The popliteus may originate from the inner aspect of the fibular head and insert above the oblique tibial line in 14% of cases. The normal origin and insertion are demonstrated in Figure 8.18. A fairly common accessory flexor muscle, the accessorius longus digitorum, arises from the lower tibia and fibula and interosseous membrane and passes anterior to the flexor retinaculum to insert with the flexor digitorum longus and quadratus plantae tendons.47 Cheung et al.77 found a 6% prevalence of the flexor digitorum accessorius longus in a group of 100 asymptomatic volunteers. Eberle et al.74 reported this accessory muscle in 8% of the population. Flexor hallucis syndrome can occur when this accessory muscle is present.
Figure 8.33 Illustration of the dorsal neurovascular anatomy of the foot. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
Several variations may cause confusion on MR or CT images. The muscles may fuse to form one unit, and occasionally the peroneus longus insertion expands to include the bases of the three to five metatarsals. An accessory peronealmuscle may arise from the fibula between the peroneus longus and brevis. Its tendon generally inserts in the peroneus longus tendon on the plantar aspect of the foot.5,47,49
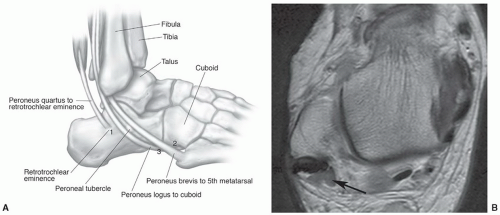
The peroneus quadratus is present in about 10% to 13% of patients.40,73,78 This anomalous muscle is three times as common in males compared with females. This arises from the posterior fibula between the longus and brevis. Three variations of the peroneus quadratus have been described based on their insertions. One of this subgroup inserts on the calcaneus (perocalcaneus externum), one on the cuboid (peroneocuboideus), and the third variation inserts on the peroneal tendon (long peroneal).47 The peroneus quadratus has been associated with clinical symptoms (pain and instability), and is associated with peroneal tendon subluxation. The peroneus quadratus tendon is posterior to the brevis and longus tendons on MRI (Fig. 8.35).47,78
Figure 8.34 Illustration of the plantar neurovascular anatomy of the foot. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.)
The peroneus digiti minimi is rare. It arises from the lower fibula and inserts on the extensor surface of the fifth toe.5,47
An important variant is the accessory soleusmuscle. This muscle bundle extends into the pre-Achilles fat (Kager’s fat pad).79,80,81,82,83 This muscle may be noted incidentally or cause clinical symptoms. Patients may present with pain after exercise or a soft tissue mass. MRI (Figs. 8.36 and 8.37) can confirm the presence of this normal variant and differentiate normal muscle from a muscle tear or neoplasm.5,74
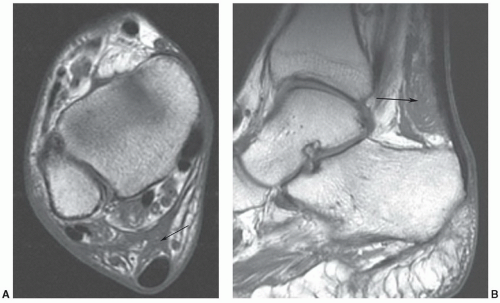
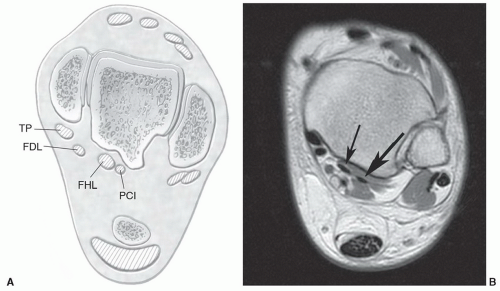
Another accessory muscle, the peroneocalcaneus internus, occurs in 1% of asymptomatic patients.84 In up to 75% of cases this accessory muscle is bilateral. The muscle arises from the lateral flexor hallucis longus and the posterior fibula. It lies posterolateral to the flexor hallucis longus as it courses inferiorly to the sustentaculum tali to insert on the calcaneus.47 Both tendons may be visible on sagittal and axial MR studies as they pass inferiorly to the sustentaculum tali (Fig. 8.38).84,85 The peroneocalcaneus internus muscle does not present as a soft tissue mass or cause neurovascular compression, which can occur with other accessory muscles.40,73,79 However, in some cases, it may displace the flexor hallucis longus muscle and may cause indirect neurovascular compression.
Figure 8.35 A: Illustration of the peroneus quadratus, which may insert on the retrotrochlear eminence (1), cuboid (2), or peroneus longus tendon (3). B: Axial MR image demonstrating peroneus quadratus (arrow) medial and posterior to the peroneus brevis and longus tendons.
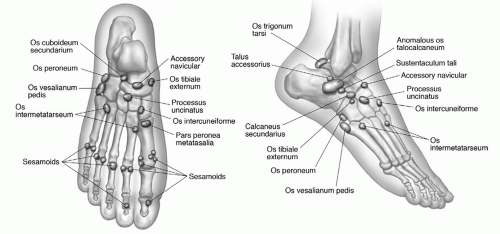
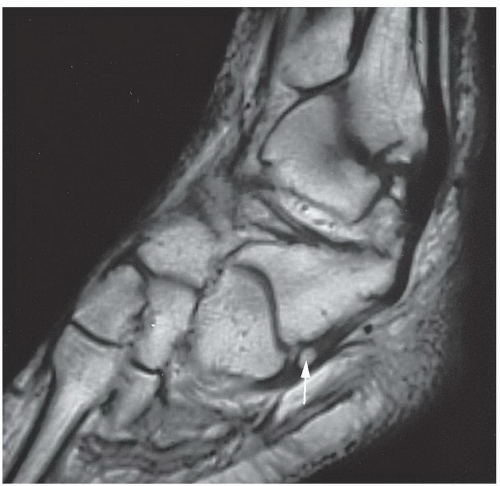
One must also be familiar with accessory ossicles and variations in bony anatomy (Figs. 8.39 and 8.40).50 Ossicles are easily detected and characterized on routine radiographs and CT. However, ossicles may cause confusion on MR images (Fig. 8.41). This is one of several reasons why it is important to compare MRI with routine radiographs before interpreting MR studies.5 Common ossicles include the accessory navicular, os peroneum, os subfibulare (Fig. 8.41), and os sustentactuli.40,73 The os sustenculi is seen in 1% of patients. The ossicle lies at the posterior margin of the sustentaculum tali. This ossicle can become symptomatic, but should not be confused with a fracture.73
Figure 8.36 Accessory soleus muscle. Axial (A) and sagittal (B) T1-weighted images demonstrating an accessory soleus muscle (arrow).
Figure 8.37 Patient with ankle pain and fullness posteriorly. Examination is performed in the head coil to allow comparison and improved detection of subtle lesions. Axial T1-weighted images of the ankles demonstrate an accessory soleus muscle on the left (A) (arrow) that may have been overlooked if the opposite ankles were not available for comparison. Note the normal pre-Achilles fat on the right (B) (arrowhead).
Figure 8.38 A: Axial illustration of the ankle demonstrating four medial tendons instead of the usual three tendons: Tibialis posterior (TP), flexor digitorum longus (FDL), flexor hallucis longus (FHL), and peroneocalcaneus internus (PCI). B: Axial T1-weighted image demonstrating peroneocalcaneus internus (large arrow) lateral to the flexor digitorum longus (small arrow). (From Bancroft LW, Bridges MD. MRI: Normal Variants and Pitfalls. Philadelphia, Lippincott Williams & Wilkins; 2008.)
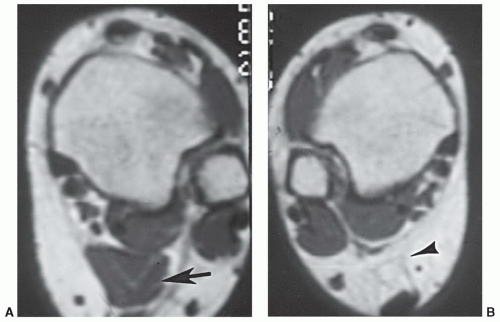
There are three types of accessory navicular. The Type I accessory navicular is round to oval and is imbedded in the distal posterior tibial tendon (PTT). Type II is more triangular and maintains a fibrocartilagenous attachment to the navicular (Fig. 8.42). Overuse can lead to symptoms at the fibrocartilagenous junction. Type III is cornuate or a prominent medial tubercle. The Type II accessory navicular is frequently seen in patients with PTT dysfunction.5,73
Figure 8.39 Illustration of ossicles in the foot. (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, Lippincott Williams & Wilkins; 2011.)
Figure 8.40 Sagittal proton density weighted image of the os peroneum (arrow).
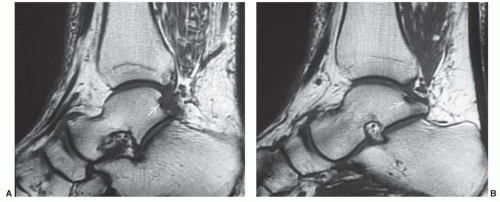
A pseudodefect in the posterior talar articular surface is a common finding on MR images (Fig. 8.43). The defect is seen as an area of irregularity at the posterior articular margin (Fig. 8.43). Signal intensity is reduced on both T1- and T2-weighted sequences. Both tali are involved in 86% of patients. The pseudodefect should not be confused with bone erosion or an osteochondral fracture.86
There are two areas of prominence on the lateral calcaneus. The peroneal tubercle is seen in 40% of the general population and is part of the fibro-osseous tunnel for the peroneal tendons. Posterior to the peroneal tubercle is the retrotrochlear eminence that is evident in 98% of patients. The accessory penoneus quadradus muscle may attach on this eminence (Fig. 8.35A).40,73,82,88
Pseudo-osteochondral defects have also been reported in the distal tibia (groove for the posterior tibiofibular ligament) and talus that should not be confused with erosions or osteochondral fractures.40,73,82,90
Noto et al.89 reviewed normal variants on MR images in 30 patients. Common variations included an irregularity of the posterior tibiotalar joint (27/30 cases), variations in signal intensity at points of tendon insertions (not to be confused with tendon rupture), and small amounts of fluid in the tendon sheath surrounding otherwise normal tendons. The latter may be particularly difficult to differentiate from early tenosynovitis.
There is normally a small amount of fluid in the tendon sheaths of the foot and ankle. This finding is more common in the flexors than the extensor.40,73 The presence of asymptomatic fluid is more common in active or athletic individuals. A small amount of fluid in the retrocalcaneal bursa is evident in 53% to 68% of patients. Increased fluid in the joints (18% to 34%) and peritendinous regions (22%) is also common.40,90,91
Figure 8.41 Sagittal T1-weighted images (A and B) demonstrating a small os subfibulare (arrow). Determining whether an abnormality or an ossicle is present can be difficult, depending on the size and marrow content of the ossicle.
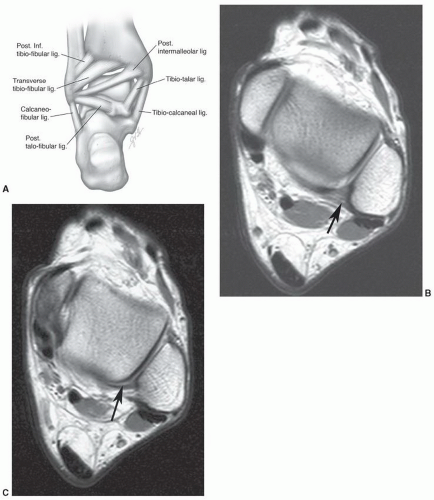
The posterior intermalleolar ligament is a normal variant that lies between the posterior tibiofibular ligament and the posterior talofibular ligament (Fig. 8.44). The posterior intermalleolar ligament has received some attention in the orthopedic literature because of its association with posterior impingement syndrome.63,92 Rosenberg et al.92 studied MR features of this ligament and found that it was most easily detected on axial or coronal images (Fig. 8.44). The ligament was identified on 19% of clinical MRI studies.92 This ligament may be more easily studied using three-dimensional GRE images.
Figure 8.42 Accessory navicular. A: Illustration of types of accessory navicular. Type I, round and separated; Type II triangular with fibrous attachment; Type III, prominent medial tubercle or cornuate navicular. B: AP radiograph demonstrating the typical Type I navicular (arrow). C: Axial T1-weighted demonstrating the insertion of the posterior tibial tendon on a Type II accessory navicular. Note the fibrous attachment (arrow). (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, Lippincott Williams & Wilkins; 2011.)
Fiorella et al.93 evaluated MRI features of the posterior intermalleolar ligament in patients with posterior impingement syndrome of the ankle. They found a prominent intermalleolar ligament as the most probable cause of posterior impingement syndrome in these patients in the absence of other structured causes. Ankle arthroscopy was performed in one of these patients in which arthroscopic resection of the intermalleolar ligament resulted in resolution of the posterior impingement syndrome in this patient.93
Figure 8.43 Sagittal T1-weighted images (A, B) demonstrating a low-signal-intensity pseudodefect near the posterior articular margin of the talus (arrow).
Partial volume effects can also create apparent abnormalities. This is a particularly significant problem when evaluating the complex ligament anatomy and the variations in signal intensity created by the “fanned” insertions andmultidirectional slips of the ligaments.5,40,88 Useofmultiple image planes can be helpful in minimizing this problem.
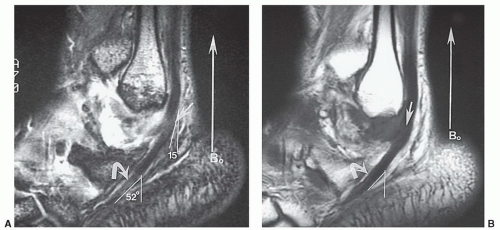
The “magic angle” effect can create apparent pathology when structures (tendons or ligaments) are oriented 55° to the magnetic field (B0).82,94,95 Signal intensity is increased maximally at 55° with intermediate signal intensity within 10° (45° to 65°) of the magic angle.95 This phenomenon is most commonly associated with short TE spin-echo or GRE sequences (Fig. 8.45). Signal intensity aberrations can also be detected at ligament or tendon insertions where diverging fibrous structures enter the magic angle.94,95 In our experience (Fig. 8.45), this phenomenon and partial volume effects can have a similar MR appearance.
CLINICAL APPLICATIONS
The applications for MRI of the calf, foot, and ankle have expanded dramatically in the last decade.1,27,62,66,90,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108 Ease of positioning, multiple image planes, and the superior contrast afforded by MR are ideal for examination of many foot and ankle disorders. In our practice, the most common applications are trauma, specifically soft tissue trauma, neoplasms, infection, osteonecrosis, nerve compression syndromes, and diabetic foot disorders.
TRAUMA
Foot and ankle injuries account for 10% or more of emergency room visits.9,29,107 Routine radiographs and conventional techniques are still best suited for evaluation of patients with acute skeletal injuries. Chronic post-traumatic syndromes and certain soft tissue injuries may be more ideally suited to MRI evaluation. Karasick et al.108 demonstrated that MRI is important for evaluating painful conditions of the forefoot when conventional radiography is not diagnostic.
FRACTURES
Most skeletal injuries are still easily detected with routine radiographs. However, subtle fractures, bone contusions, and complete assessment of fracture patterns, physeal, and associated soft tissue injuries is more easily accomplished with MRI.4,5,7,20,111 Subtle marrow injuries (bone bruises and marrow edema) can be detected that may go undiagnosed with conventional imaging techniques (Figs. 8.46 and 8.47).103,109,110,111,112
Bone marrow edema pattern and bone bruises may occur in multiple settings. Areas of low signal intensity on T1- and high signal intensity on T2-weighted and STIR sequences are commonly seen in the foot.114 The etiology is unclear, but may be traumatic or related to stress response (Fig. 8.48).110,112
Marrow edema pattern is not specific, especially in children. Pal et al.113 reported abnormal signal intensity on T1- and T2-weighted images in children. Fifty-seven per cent of these patients were asymptomatic. Findings in asymptomatic patients were attributed to normal growth and marrow conversion.113 Follow-up studies in children demonstrate that marrow signal intensity changes return to normal by age 15 years indicating they may be related to red marrow conversion.114
Figure 8.44 Posterior intermalleolar ligament. (A) Posterior illustration. Axial T1-weighted (B and C) and coronal DESS image (C) demonstrating the intermalleolar ligament (arrow). (From Berquist TH. Imaging of the Foot and Ankle. 3rd ed. Philadelphia, Lippincott Williams & Wilkins; 2011.)
Bone bruises are typically associated with acute trauma. Seven to 25% of patients with ankle sprains have associated bone bruises.115 Axial loading injuries can result in bilateral calcaneal bone bruises.109 Bone bruises have a similar appearance to marrow edema pattern. Signal intensity changes are likely related to microfracture and hemorrhage. A complete fracture can result if continued stress is applied to the involved area.20,103
Stress fractures and insufficiency fractures are common in the foot and ankle. The formeris related to repetitive stress to normal bone structure. Insufficiency fractures occur when normal stress is applied to abnormal bone.5,20,111 In the foot, stress fractures most commonly involve the second through fourth metatarsal shafts and necks (Fig. 8.49). The metatarsal bases are more commonly involved in ballet dancers.116,117 The navicular and base of the fifth metatarsal may also be involved.116,117 Stress response is the first stage of stress fractures.20,110 Edema, hyperemia, and increased osteoclastic activity in the involved region show a poorly defined area of signal abnormality with low signal intensity on T1- and high signal intensity on T2-weighted or STIR sequences.20,110 Over time, a linear fracture line may be evident, especially in the navicular and calcaneus (Figs. 8.46 and 8.50). Periosteal callus tends to form early around metatarsal stress fractures (Fig. 8.49C). This can be easily identified on axial and coronal or sagittal MR images. MRI is more sensitive and specific than radionuclide scans, particularly in the elderly or osteopenic population.20,111
Figure 8.45 Gradient echo (A) and T1-weighted (B) sagittal images of the peroneal tendons in a patient with synovitis and areas of increased signal intensity in the tendon proximally (straight arrow) and inferiorly (curved arrow). The angle of the tendon is 52° inferiorly and increased signal is due to magic angle effect. Partial volume effects create increased signal proximally due to inflammation in the adjacent tissues.
Figure 8.46 Patient with midfoot pain and normal radiographs. Sagittal T1- (A) and T2-weighted (B) and axial T2-weighted (C) images demonstrate marrow edema and a fracture in the navicular (arrow). The axial image (C) more clearly demonstrates the fracture.
Figure 8.47 Sagittal proton density-weighted image of a subtle calcaneal fracture (arrow).
Figure 8.48 Stress response. Fat-suppressed T2-weighted fast spin-echo axial (A) and coronal (B) images demonstrate marrow edema in the proximal second metatarsal without cortical disruption.
Arendt and Griffiths118 graded stress injuries based upon the MR image appearance and the degree of marrow, cortical, and periosteal involvement. Grade 0 is normal. Grade 1 injuries demonstrate periosteal edema without marrow signal abnormality. Grade 2 injuries demonstrate periosteal and marrow edema. Grade 3 changes are similar to Grade 2, but are more defined (Fig. 8.51). Grade 4 injuries demonstrate findings similar to Grade 3, but with a discrete fracture line (Fig. 8.52).
Robbins et al.119 found that MR was valuable in detecting subtle fractures of the anterior calcaneal process. If these fractures are not immobilized early, painful nonunion may result. Marrow edema confined to the anterosuperior calcaneal process is consistent with a bifurcate ligament avulsion. Marrow edema seen in both the anterosuperior calcaneal process and the cuboid is an impaction type fracture called the “nutcracker lesion,” which is seen in athletes such as gymnasts.119
Osteochondral fracture can be related to an acute injury or chronic repetitive trauma (osteochondritis dissecans).20,120,121 Both lesions are easily detected and classified using MRI. The talar dome (Fig. 8.53) is most commonly involved and accounts for 4% of cases of osteochondritis dissecans.120
Berndt and Harty122 classified osteochondral lesions of the talar dome based upon cartilage integrity and fragment position. Stage I lesions involve subchondral bone with intact cartilage. Stage II lesions have partially detached osteochondral fragments, and stage III lesions are completely detached but undisplaced. Stage IV lesions are completely detached and displaced (Figs. 8.54 and 8.55). MRI is useful in classifying talar dome injuries, and using axial and coronal images define the site and size of the lesion (Figs. 8.56 and 8.57
Only gold members can continue reading. Log In or Register to continue