pronation and supination are also useful for evaluating the biceps tendon and subtle abnormalities in the radioulnar joint. Both axial and sagittal images should be obtained. When motion studies are required, we have used gradient echo (GRE) sequences (see below) and cine studies. Quick et al.13 used fast imaging steady state precession (FISP) sequence to perform motion studies of the elbow and other joints. True FISP is a steady state precession GRE sequence. The parameters used in this study include repetition time/echo time (TR/TE) of 2.2/1.1 ms, flip angle (FA) 50°, field of view (FOV) 12 to 27 cm, section thickness of 6 mm, and a 256 × 135 matrix.13
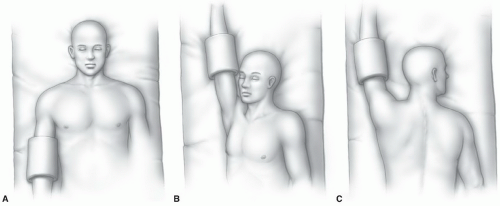 Figure 10.1 Illustration of positions for imaging the elbow. Positioning the arm (A) at the side is most comfortable for the patient. When the arm is positioned (B, C) above the head, the patients have more difficulty tolerating the examination. The patient is rotated in B, which is often necessary with larger patients or when elbow flexion is needed to evaluate the biceps tendon. |
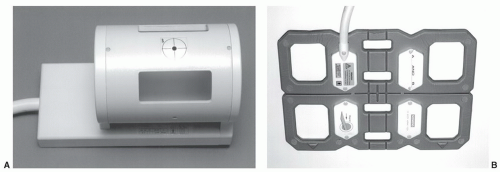 Figure 10.2 Photographs of the elbow (A) and larger phased-array (B) coils. |
the elbow. Signal to noise ratios and spatial resolution were improved compared to conventional coil techniques.18
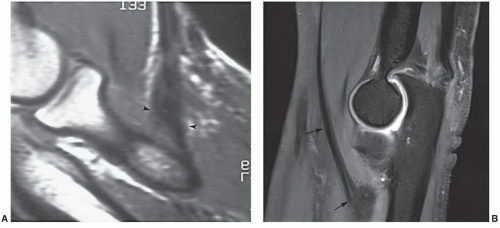 Figure 10.3 Normal distal biceps tendon. A: Sagittal 1.5-T T1-weighted image with the elbow flexed demonstrates the biceps tendon as it expands (arrowheads) near its attachment on the tuberosity of the radius. B: Properly rotated 3.0-T turbo spin-echo fat-suppressed T2-weighted image clearly demonstrates the biceps tendon (arrows) to the level of the radial tuberosity. |
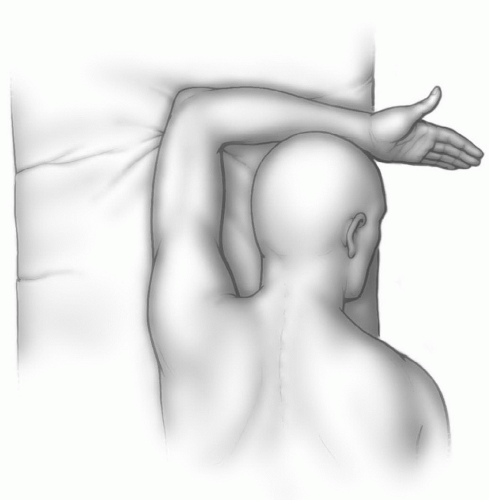 Figure 10.4 Illustration of the flexed abducted supinated view for evaluation of the biceps tendon. The thumb is up. |
the coronal and sagittal planes (Table 10.1). We also obtain dual echo steady state (DESS) images in the coronal plane using 1-mm sections to better evaluate the articular cartilage and collateral ligaments. Coronal and sagittal images are oriented based upon the position of the epicondyles (Fig. 10.6).
Table 10.1 Routine Examination MRI of the Elbow and Forearm at 1.5 T | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
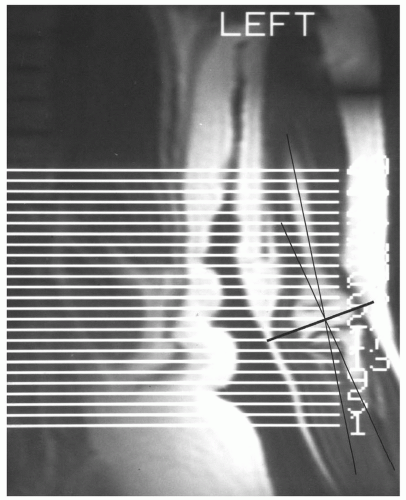 Figure 10.5 Coronal scout image of the elbow with axial image planes selected. The left side of the trunk is also seen due to the large (40 cm) field of view. The axis of the humerus and forearm (dark lines) must be considered to obtain true axial images. The normal carrying angle of the elbow is 3° to 29°. Therefore, axial images of the forearm need to be angled (black transverse line). |
that pain, if present, is intra-articular. Following injection, fat-suppressed T1-weighted images are obtained in the axial, coronal, and sagittal planes. In addition, we obtain T2-weighted fat-suppressed FSE images in the coronal plane to better evaluate the capsule and collateral ligaments.
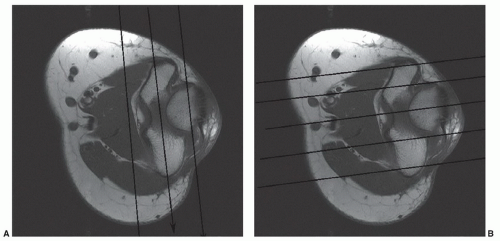 Figure 10.6 Axial T1-weighted images with coronal (A) and sagittal (B) planes aligned with the epicondyles. |
recesses are deep in the respective UCL and RCL. Synovial folds of various sizes and shapes normally project into the joint space and should not be mistaken for intra-articular loose bodies.27 These synovial folds usually occur at the junction of two synovial recesses or a triangular meniscuslike structure at the joint line margin.27
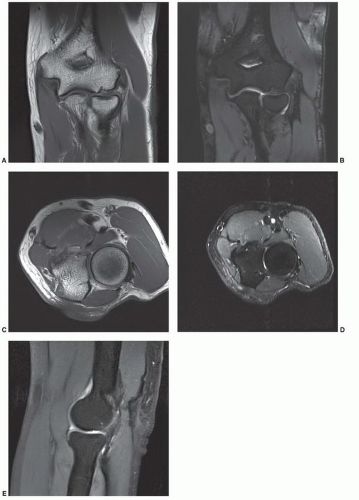 Figure 10.7 Commonly used pulse sequences for the elbow. 3.0 T coronal T1-weighted (A) and DESS (B) sequences. The DESS sequences are particularly useful for demonstrating articular cartilage. Axial T1- (C) and fat-suppressed turbo spin-echo T2-weighted (D) images. E: Sagittal fat-suppressed turbo spin-echo T2-weighted image. |
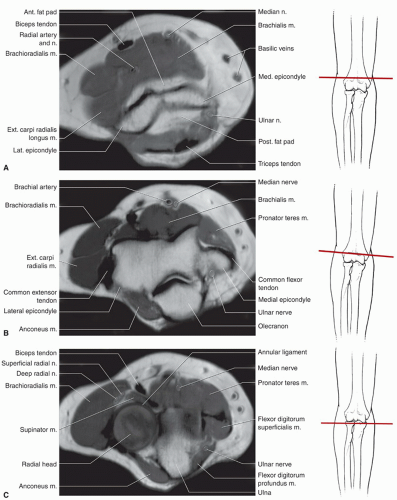 Figure 10.8 Axial proton density-weighted MR images with anatomy labeled and illustration demonstrating the level of section. A: Axial image through the supracondylar region. B: Axial image through the medial and lateral epicondyle. C: Axial image through the radial head. D: Axial image at a level just distal to the radial head. E: Axial image at the level of the radial tuberosity. F: Axial image below the tuberosity level. G: Axial image of the proximal forearm. |
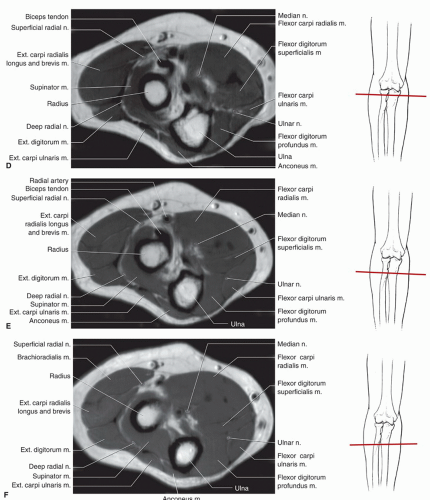 Figure 10.8 (continued) |
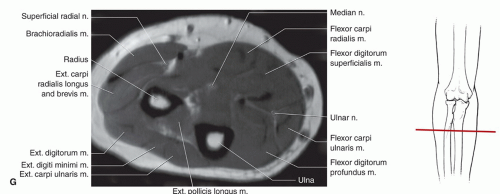 Figure 10.8 (continued) |
surface of the epicondyle to attach the medial edge of the coronoid process (Fig. 10.14A). The posterior band is smaller and has a fan-like configuration.25 It extends from behind the medial epicondyle and courses slightly posteriorly to attach onto the medial aspect of the olecranon (Fig. 10.14A). The transverse band is clinically less significant, small, or sometimes absent, and is often difficult to identify on MRI.2,3,30
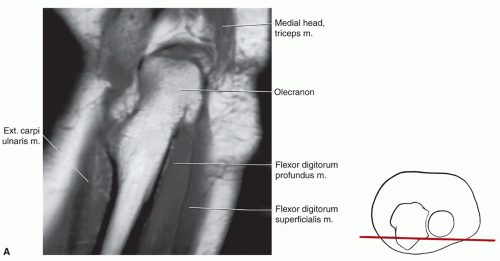 Figure 10.9 Coronal image of the elbow and forearm with anatomy labeled and illustration demonstrating the section level. A: Coronal image through the posterior elbow and forearm. B: Coronal image through the mid elbow and forearm. C: Coronal image through the anterior elbow and forearm. |
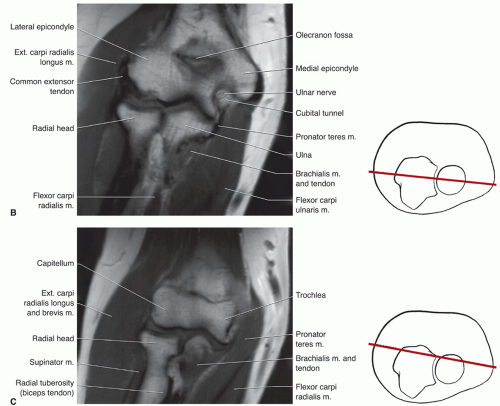 Figure 10.9 (continued) |
subcutaneous olecranon bursa. There are also intratendinous and subtendinous bursae in the olecranon region (Fig. 10.16) (Table 10.2).28,34 The subtendinous bursa (bicipitoradialis) is best seen on axial and sagittal MR images and should not be confused with an elbow effusion. An inflamed bursa can be differentiated from a simple effusion by the lack of fluid in the anterior compartment of the elbow. The other two superficial bursae, the medial epicondylar and lateral epicondylar, should not be confused with disruptions or tears in the medial and lateral collateral ligaments. Figure 10.17 demonstrates the location of the other superficial and deep bursa in the elbow region. The relationship of these bursae to branches of the radial and ulnar nerves (Fig. 10.17) is important.27,34 These bursae are normally
not identified, but when inflamed and fluid-filled (due to trauma, infection, synovitis, or gout), they can be demonstrated on T2-weighted or GRE images.5 In this setting, the bursae will appear as homogeneous, high intensity structures with clearly defined margins.1,2
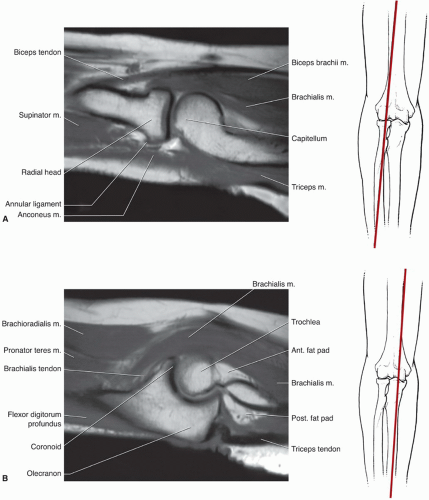 Figure 10.10 Sagittal images of the elbow and forearm with anatomy labeled and illustration demonstrating the section level. A: Sagittal image through the lateral radiocapitellar joint. B: Sagittal image through the ulnar-trochlear articulation. |
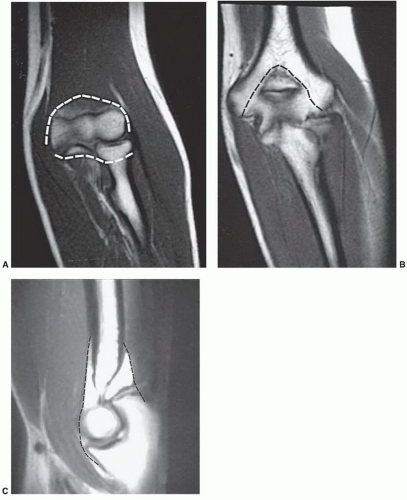 Figure 10.11 MR images of the capsule of the elbow (broken lines) seen on coronal T1-weighted images anteriorly (A) and posteriorly (B) and sagittal (C) image. |
brachioradialis (Figs. 10.8, 10.10, and 10.18) (Table 10.3). The biceps brachii crosses the elbow anteriorly to insert onto the radial tubercle and serves as a supinator and flexor (Figs. 10.3, 10.8, and 10.18).27 The brachialis is a large muscle that arises from the anterior humerus and passes anterior to the elbow before inserting onto the proximal ulna near the coronoid process (Figs. 10.8, 10.9, 10.18, and 10.19). The brachioradialis arises from the radial side of the distal humerus (Fig. 10.18), crosses the lateral epicondyle, and extends distally to insert just proximal to the metaphysis of the radius (Figs. 10.8, 10.9, 10.10). In its activity as a flexor, the brachioradialis is aided by the adjacent muscles of the extensor group, especially the extensor carpi radialis longus.3,27,34 A fourth and less important flexor of the elbow is the pronator teres, which functions optimally only when the forearm is pronated. The pronator teres arises from the supracondylar
portion of the humerus, extends obliquely across the medial aspect of the elbow, and inserts onto the upper third of the radius (Figs. 10.8, 10.9, and 10.18).27,34
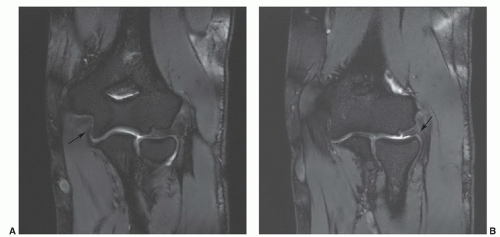 Figure 10.12 Coronal DESS images at 3.0-T demonstrating the ulnar (arrow in A) and radial (arrow in B) collateral ligaments. |
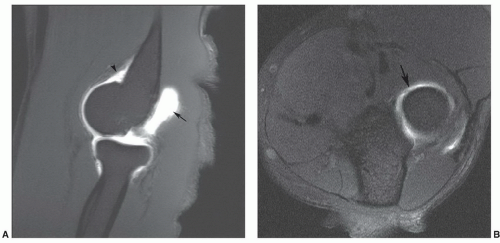 Figure 10.13 Recesses of the elbow. A: Sagittal MR arthrogram image demonstrating the olecranon (arrow) and anterior humeral (arrowhead) recesses. B: Axial MR arthrogram image demonstrating the annular recess. (Courtesy of Jeffrey J. Peterson MD, Mayo Clinic Florida.) |
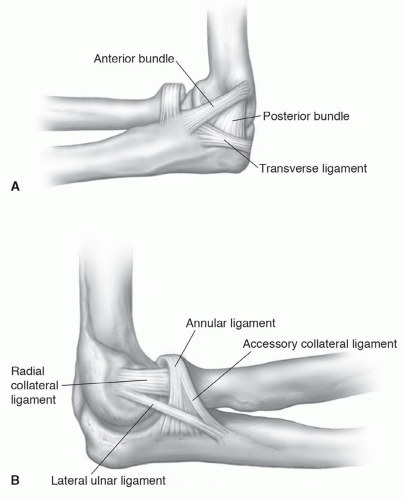 Figure 10.14 Lateral illustrations of the ligaments of the elbow from the medial (A) and lateral (B) sides. |
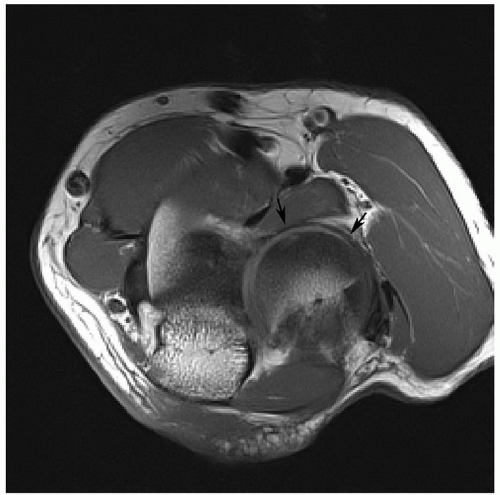 Figure 10.15 Axial T1-weighted 3.0 T image demonstrating the annular ligament (arrows). |
groove, and the lower posterior humerus.27,34 It inserts onto the olecranon. The anconeus (Figs. 10.8 and 10.20) arises from the posterior lateral epicondyle and extends distally and medially to insert onto the lateral ulna (Fig. 10.20).
Table 10.2 Elbow Bursae | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
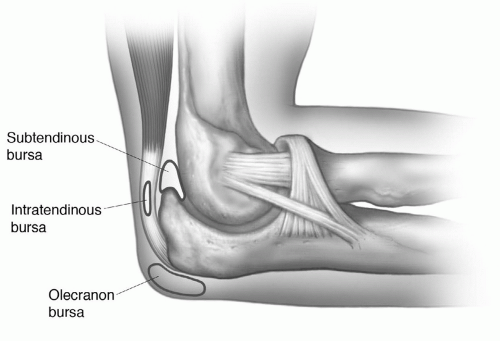 Figure 10.16 Illustration of the olecranon bursae. The superficial subcutaneous bursa is most commonly seen. The intratendinous and subtendinous bursae are less frequently identified. |
Table 10.3 Muscles of the Elbow | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
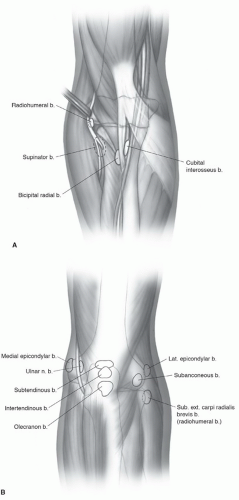 Figure 10.17 Illustrations of the bursae of the elbow as seen (A) anteriorly and (B) posteriorly. Note the relationship of the bursae to the ulnar nerve and neural branches anteriorly. T2-weighted sagittal (C) and axial (D) images in a patient with olecranon bursitis demonstrate fluid distending the olecranon bursa (arrows). |
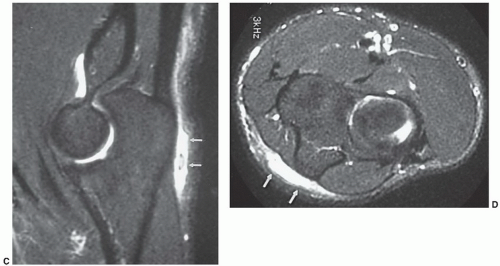 Figure 10.17 (continued) |
the wrist through the pisohamate and pisometacarpal ligaments to insert onto the hamate hook and fifth metacarpal base.27,29,30
Table 10.4 Muscles of the Forearm | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
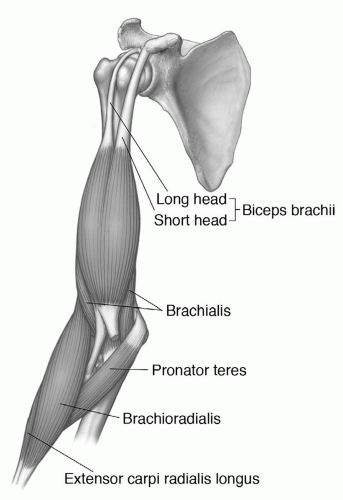 Figure 10.18 Illustration of the superficial flexor muscles of the elbow. |
flexor retinaculum, the flexor digitorum superficialis gives off four tendons. After passing through the flexor retinaculum and carpal tunnel, these four tendons have common sheaths with the flexor digitorum profundus and split distally to insert onto either side of the bases of the second through fifth middle phalanges.27,29,30,34
 Figure 10.19 Sagittal 3.0-T fat suppressed proton density weighted image demonstrating the insertion of the brachialis muscle/tendon near the coronoid process of the ulna (arrow). |
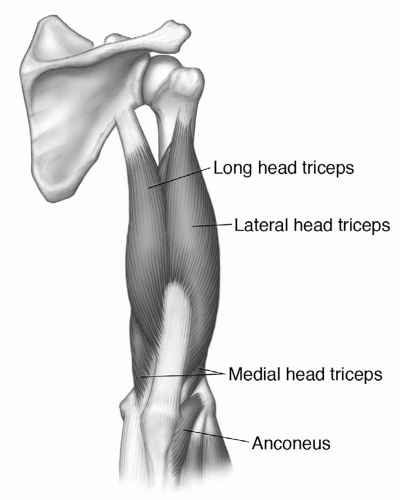 Figure 10.20 Illustration of the extensors of the elbow. |
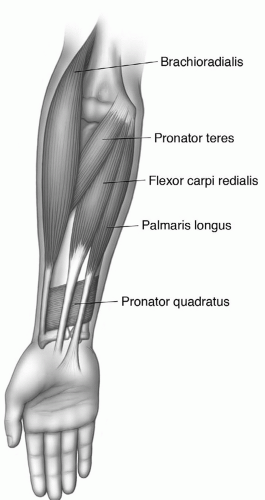 Figure 10.21 Illustration of the pronators of the forearm. |
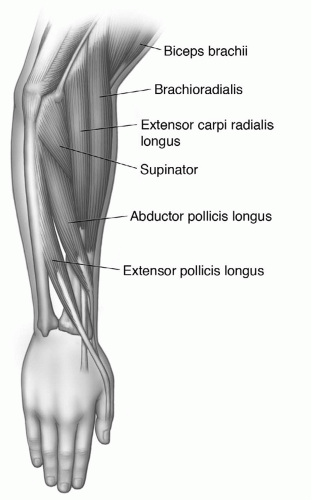 Figure 10.22 Illustration of the supinators of the forearm. |
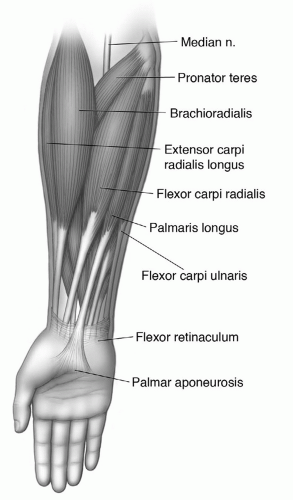 Figure 10.23 Illustration of the superficial flexor and extensor muscles of the forearm. |
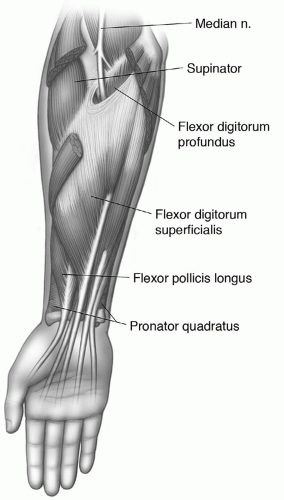 Figure 10.24 Illustration of the intermediate flexor compartment of the forearm. |
digitorum longus and flexor pollicis longus. This muscle arises from the distal ulna to insert onto the distal radius in a near-transverse direction (Fig. 10.25).27,28,29,34
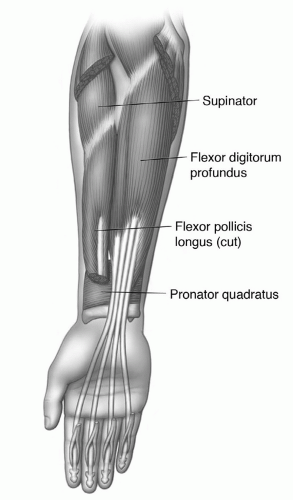 Figure 10.25 Illustration of deep flexors of the forearm. |
portion of the dorsal forearm. It originates from the common extensor tendon and shares an origin with the belly of the extensor digiti minimi. Distally, three to four tendons are present with a common sheath within the extensor retinaculum. The sheath is shared with the extensor digiti indicis. The tendons pass under the extensor retinaculum and receive slips from the lumbricals and interosseous muscles in the hand, thereafter dividing into central and lateral bands (see Chapter 11). The central bands insert onto the middle and lateral bands on the sides of the distal phalanges. The primary function of the extensor digitorum is to serve as an extender and abductor of the fingers. The extensor digiti minimi arises largely from a septum adjacent to the extensor digitorum and occupies a superficial position on the dorsal forearm between the extensor digitorum and extensor carpi ulnaris. The slender tendon of this muscle continues in a separate compartment under the extensor retinaculum to insert onto the dorsal aspect of the small finger in a similar fashion to the extensor digitorum. The extensor carpi ulnaris is the most medial of the superficial muscles. It has two heads, the first arising from the lateral epicondyle via the common extensor tendon, and the second from the posterior border of the ulna. The tendon of this muscle passes through a special compartment in the extensor retinaculum and also through the ulnar groove. The insertion is the medial side of the base of the fifth metacarpal. Its primary functions are wrist extension and ulnar abduction.27,29,30,34
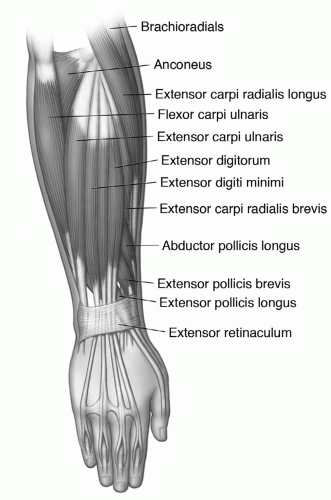 Figure 10.26 Illustration of extensor muscles of the forearm. |
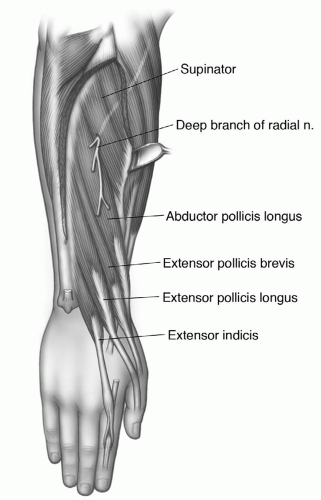 Figure 10.27 Illustration of the deep extensor muscles of the forearm. |
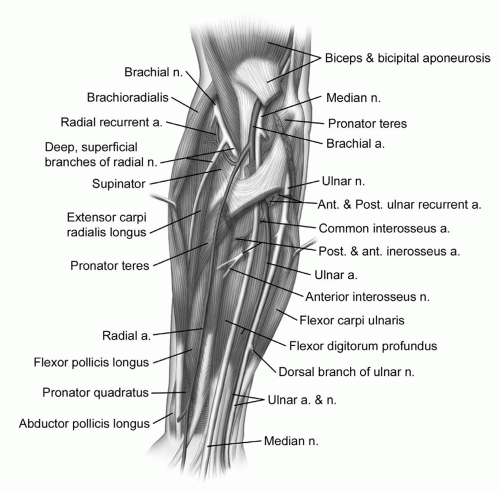 Figure 10.28 Illustrations of the neurovascular anatomy of the elbow and forearm. |
usually accompanies the median nerve along its course superficial to the flexor digitorum profundus. Figure 10.28 demonstrates the major neurovascular anatomy of the forearm and elbow.27,41 Figure 10.29 depicts the normal MR angiogram of the elbow and proximal forearm.
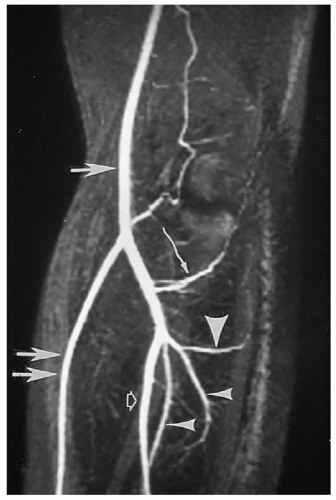 Figure 10.29 Normal MR angiogram of the elbow and proximal forearm. The distal brachial artery (large arrow), proximal radial (large double arrows), and ulnar (open arrow) arteries are illustrated. The proximal portions of the anterior and posterior ulnar recurrent arteries (curved arrow), anterior and posterior interosseous arteries (small arrowheads), and posterior interosseous recurrent artery (large arrowhead) are well visualized. |
ridge in the trochlear notch that is not covered with hyaline cartilage. This finding is most easily appreciated on sagittal images and should not be mistaken for a cartilage lesion (Fig. 10.31).44
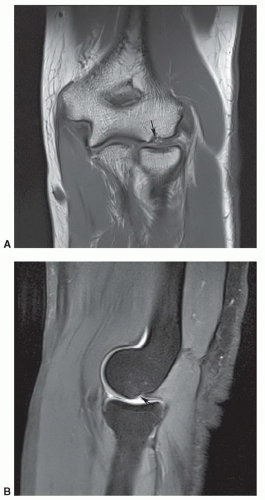 Figure 10.30 Capitellar pseudodefect. Coronal T1-weighted (A) and fat suppressed proton density turbo spin-echo T-2 weighted (B) images demonstrating the normal variant. There is no marrow edema to suggest active impaction. |
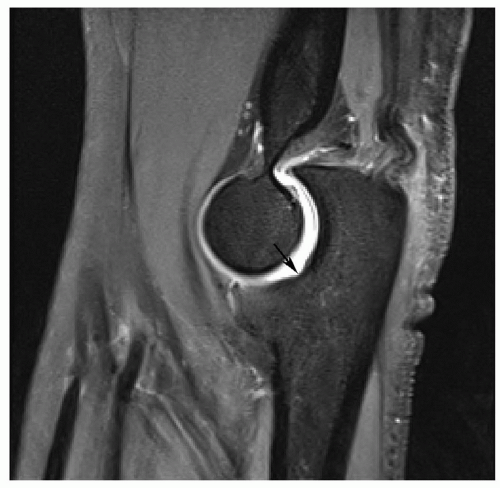 Figure 10.31 Trochlear notch. Sagittal turbo spin-echo fat-suppressed proton density image demonstrating the normal trochlear notch (arrow). |
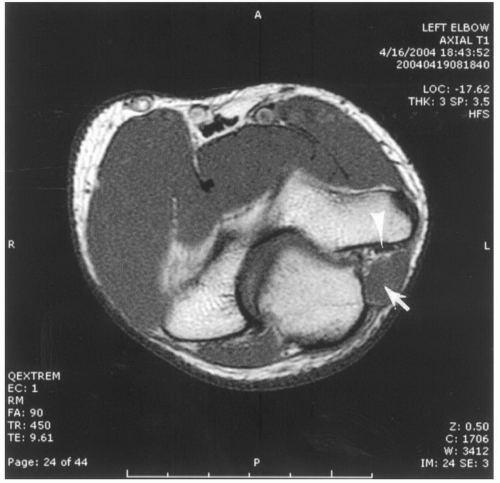 Figure 10.32 Axial T1-weighted image of the elbow demonstrates an anconeus epitrochlearis (arrow) compressing the ulnar nerve (arrowhead). |
however, it is still useful to change the phase encoding direction to prevent artifacts from degrading important areas on the image (Fig. 10.33).1,2,53
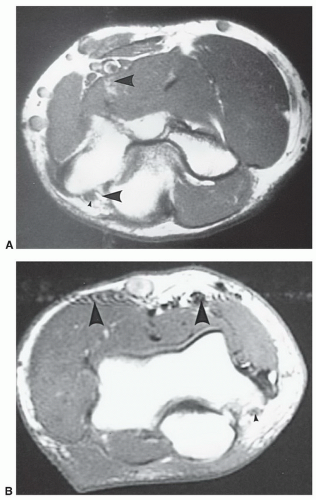 Figure 10.33 Flow artifact. Axial images of the elbow showing flow artifact in the (A) vertical y-axis and (B) transverse or x-axis. The ulnar nerve region (small arrowhead) is distorted by flow artifact (large arrowheads) in A, which could interfere with diagnosis of pathology in this region. |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


