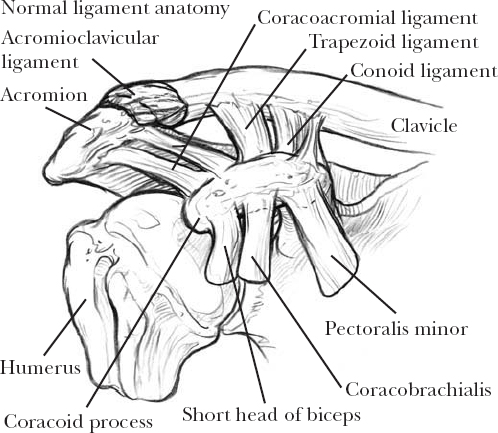
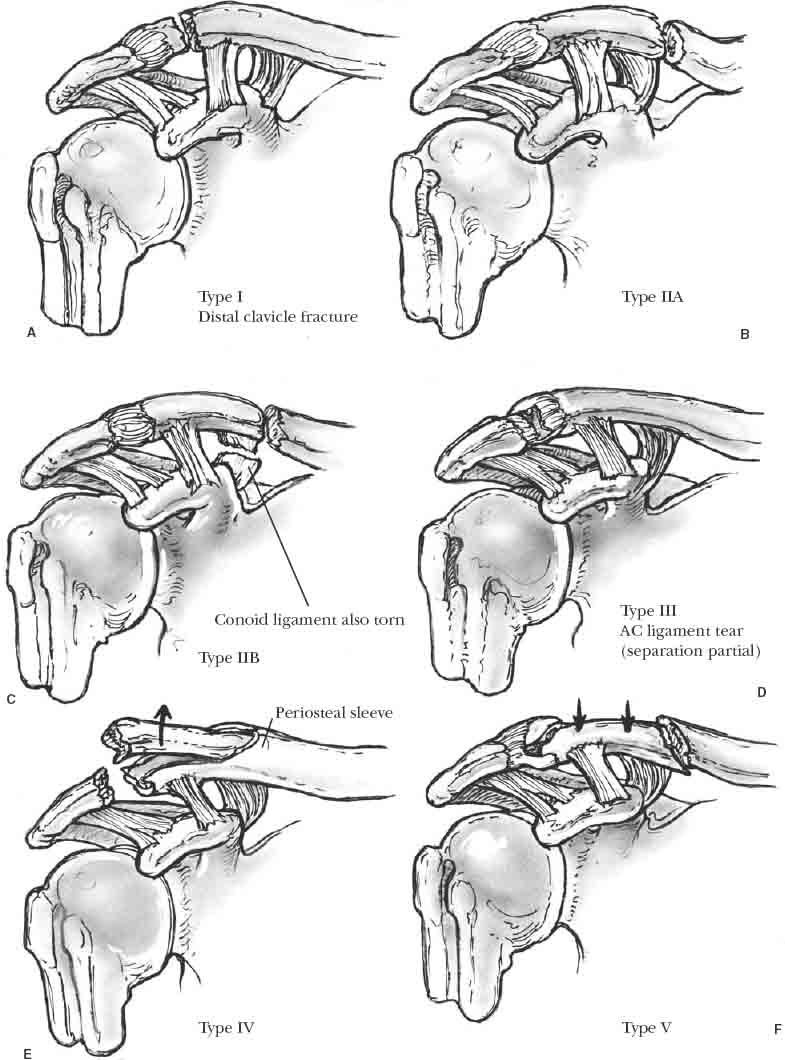
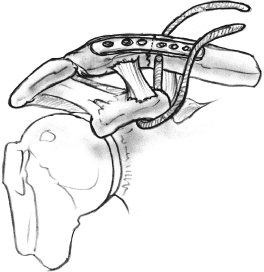
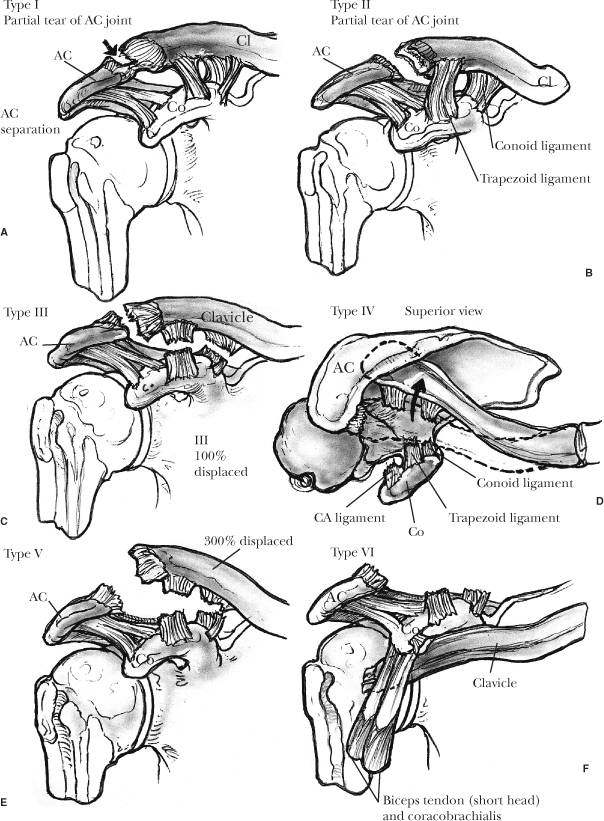
12 Injuries to the distal clavicle and acromioclavicular joint frequently fare well with minimal intervention and conservative management. However, depending on the degree of failure of the key components involved in supporting the full weight of the upper extremity during everyday and sporting activities, these injuries can be quite disabling if neglected. Although nonoperative management is usually indicated in the majority of both injury types, this chapter aims to provide a logical nonoperative and operative treatment approach based on the degree of instability noted on clinical and radiographic evaluation. When indicated, operative treatment techniques are directed at restoring stability to the lateral clavicle and acromioclavicular joint through both osteosynthesis and ligamentous reconstruction. Application of these methods requires a sound understanding of the normal and pathological anatomy of the region along with the minimum structural requirements for supporting the mobile upper extremity. Therefore, this chapter begins with a review of regional anatomy and shoulder mechanics. Classification and treatment of distal clavicle and acromioclavicular injuries will then be discussed separately, followed by complications and results of treatment for both. Any discussion of the management of distal clavicle or acromioclavicular (AC) joint injuries assumes a thorough understanding of the anatomy and mechanical role of the structures involved. A brief review based on classic and more recent studies will focus treatment principles toward safe restoration of the critical components for shoulder function. Because the clavicle acts as the beam supporting the weight of the upper extremity and thereby linking it to the axial skeleton, significant support is required to both keep it suspended and provide a stout link to the weighted scapula. The sternoclavicular ligaments are mainly responsible for supporting the lateral clavicle and maintaining its horizontal alignment without sagging. The trapezius, originating posteriorly from the axial skeleton, also provides dynamic support through its insertion onto the superolateral clavicle and out onto the acromion and scapular spine. The static linkage between the clavicle and the upper extremity comes from the coracoclavicular ligaments and acromioclavicular ligaments. The coracoclavicular ligaments originate from the base of the coracoid process and insert on the under-surface of the distal clavicle (Figure 12-1). Specifically, the conoid ligament comes off the posteromedial base of the coracoid to insert on its tubercle in the posterior aspect of the lateral bend of the clavicle. The trapezoid originates from the coracoid base just anterolateral to the conoid and attaches to the clavicle anterolateral to the conoid insertion. The AC joint is a diarthroidal joint measuring about 9 by 19 mm with minimal inherent bony stability. The AC ligaments originate from the end of the clavicle and blend with the capsule to insert laterally onto the acromion. They consist of superior, inferior, anterior, and posterior ligaments, with the superior posterior portion being the most substantial. FIGURE 12-1. Normal ligamentous anatomy of the shoulder. With full shoulder elevation, the clavicle undergoes about 30 degrees elevation, 35 degrees posterior translation, and 50 degrees rotation. As the clavicle elevates, it passively rotates the scapula through the linkage of the coracoclavicular ligaments onto the coracoid. While the coracoid is rising with the clavicle, the scapular body is rotating up and around the thorax. Most of the clavicular rotation occurs through the sternoclavicular joint, but there is some debate as to how much rotation actually occurs through the AC joint. Inman et al1 suggested that there was 20 degrees of rotation at the joint, but others have suggested 5 degrees or less. That there could be such little motion at the joint is supported by the fact that, with a firmly placed coracoclavicular screw providing a functional claviculoscapular arthrodesis, full elevation of the shoulder remains intact.2 Although these ligaments do have a role in synchronizing motion for the shoulder, their main role is to support the AC joint. Fukuda et al3 demonstrated in cadavers that the AC ligaments are the primary restraints for posterior displacement of the clavicle and posterior axial rotation. The conoid ligament resists superior displacement and anterior superior rotation. The trape-zoid restrains compression of the joint along the longitudinal axis of the clavicle. During smaller displacements, the AC ligaments actually also restrain superior clavicular migration, whereas the conoid is more involved with this in larger displacements. Recent work by Debski et al4 suggests that with failure or division of the acromioclavicular ligaments and capsule, there is a significant increase in the forces placed on the remaining coracoclavicular ligaments and an increase in antero-posterior translation at the joint. Previous epidemiological studies have shown that clavicle fractures occur mostly in young men and constitute 5 to 10% of all fractures and 44% of all injuries to the shoulder girdle. The incidence of distal clavicle fractures is estimated to be between 12 and 15% of all clavicle fractures.5–10 Although the majority of these fractures are non-displaced and as such are treated nonoperatively, fractures with initial displacement have done poorly with this form of treatment.11 Neer12 was the first to recognize that displaced distal clavicle fractures, as a group, showed a higher nonunion rate than other areas of the clavicle. He and others reported that distal clavicle fractures accounted for over half of all nonunited clavicle fractures.9–12 Other studies have shown the prevalence of delayed union to be as high as 65% and the incidence of nonunion between 22 and 33%.8–13 Neer13 attributed these nonunions to several factors including the degree of trauma to the affected extremity, the instability of the fracture, and the difficulty with inadequate external immobilization. These features led Neer and others to recommend surgical stabilization for displaced distal clavicle fractures.9–11,14,15 Following descriptions by Allman,16 Rowe,8 and Neer,13 the clavicle has been divided into thirds for the purpose of classification.5,7,11,16,17 Neer13 recognized that distal clavicle fractures warranted a separate classification system based on his series of clavicular nonunions. He originally proposed a classification into three types. Rockwood et al2 recommended further division of type II fractures into IIA and IIB, depending on fracture location relative to the coracoclavicular ligament attachments. Craig17 added two more types of distal clavicle fractures: type IV in children and type V occurring in adults. Types I and III distal clavicle fractures may be treated with a sling, a figure-eight splint, or a harness-type device. These fractures are minimally displaced or nondis-placed, and the coracoclavicular ligaments are intact. The immobilization ends when pain and edema have subsided around 2 to 3 weeks and the patient begins gentle range of motion exercises. Full activity is allowed when complete radiographic and clinical union is evident. Recovery is usually rapid, and late complications occur in a small percentage of patients.18,19 Treatment of type II distal clavicle fractures remains controversial. Although some authors maintain that these fractures heal with nonoperative treatment,20 the majority recommend open reduction and internal fixation.6,8,12,13,17,21,22 The multiple fixation options include intramedullary fixation by threaded or nonthreaded Kirschner wires, Steinmann pins, Knowles pins, modified Hagie pins, Rush nails, or Küntscher nails. Kirschner wires with wire loop cerclage or tension band wires, fixation with plate and screws, coracoclavicular screws, and external fixation have also been described. Each technique carries its own inherent risk of complications.23 Our preference for treatment of type II distal clavicle fractures is surgical management. After evaluation of preoperative radiographs and/or CT, the size of the distal fragment will determine the type of internal fixation we choose. If the distal fragment is too small to hold any type of internal fixation, we recommend excision of the distal fragment and a modification of the Weaver-Dunn procedure.24 If the fracture fragment is large enough, we prefer open reduction and internal fixation in accordance with the AO group, using a four-to five-hole pelvic reconstruction plate with its lower profile. However, we have also used a 3.5 mm dynamic compression plate (Figure 12-3) or a small fragment T plate. A minimum of eight cortices of fixation is recommended across the fracture site to ensure adequate fixation. Repair of the coracoclavicular ligaments is also done at this time, using a nonabsorbable cerclage technique for augmentation. We also have fixed the fracture using a tension band technique using 0.062-inch Kirschner wires with either 18-gauge wire or, preferably, Arthrex Fiber-wire (Arthrex, Naples, FL). This is done in an outpatient setting making use of an interscalene block on all patients who are eligible. The interscalene block is placed in the preoperative holding area prior to the surgical procedure by the anesthesiologist. We have found this to be a key asset for postoperative pain control and patient satisfaction. Intravenous antibiotics are administered prior to the interscalene block. The patient is placed supine on the operating table for anesthetic induction and is then shifted to the beach chair position, with careful attention to pad all bony prominences. The lower body is flexed, and two large pillows are placed under the thighs and knees. Prior to prepping, two nonsterile U-shaped drapes are placed superiorly and inferiorly, providing access to the entire upper extremity from the sternoclavicular joint, above the nipple to the midaxillary line. The affected extremity is then prepped to include the hand. Once prepped, the draping is repeated with two sterile U-shaped extremity drapes, and the hand and forearm are draped with a sterile stockinette. The surgical area is then bordered with an adhesive drape to seal off the axilla. FIGURE 12-2. Classification of distal clavicle fractures. (A). Type I. (B). Type IIA. (C). Type IIB. (D). Type III. (E). Type IV. (F). Type V. FIGURE 12-3. Plate fixation of distal clavicle fracture. The incision is made in line with the clavicle anterior and inferior to the distal clavicle beginning 1 cm lateral to the AC joint. The incision can be extended as needed by carrying the incision through the skin and subcutaneous tissue. The suprascapular nerves are isolated and protected. It is important to develop thick skin flaps. The deltotrapezial fascia is then incised sharply in line with the clavicle. Subperiosteal anterior and posterior deltotrapezial fascial flaps are raised off the clavicle with a periosteal elevator, leaving tissue for a firm closure and secure reattachment of both the trapezius and deltoid at the end of the procedure. The surgeon should be careful to avoid neurovascular structures located inferior and posterior to the clavicle. This is important during both drilling and screw placement. Small Bennett retractors placed subperiosteally not only provide exposure but also help protect surrounding soft tissue structures. With further dissection, it is important to avoid not disrupting existing fracture lines, the AC ligaments, or the attached coracoclavicular ligaments. After hematoma is removed and the fracture is defined, a decision is made to proceed with plate fixation, Kirschner wires, or a tension band construct. If the distal fracture is large enough to support a plate and screws, we proceed as follows. If the coracoclavicular ligaments remain attached to the distal fragment as in type IIA, they are left intact. In type IIB fractures, the conoid is detached, and the trapezoid ligament is intact. Although it is often difficult to repair this ligament, if the anatomy is such that a repair is possible, we will suture this ligament into the clavicular periosteum or the clavicular insertion of the trapezoid ligament using a number 1 non-absorbable suture. Next, the fixation of the clavicle should be prepared. Using a small periosteal elevator, the surgeon subperiosteally dissects around the neck of the coracoid. It is important to stay posterior to the CA ligament and as close to the base of the coracoid as possible. This prevents damage to the neurovascular structures and migration of the suture. Using a curved gallbladder-type clamp, Mersilene (Ethicon, Somerville, NJ) tape (number 5) is passed under the origins of the conjoined tendon. Staying as close to the base of the coracoid as possible, the surgeon seats the Mersilene tape by holding both ends and pulling back and forth in a sawing motion. This prevents the interposition of soft tissue in the area beneath the tape. The tape is then passed with the aid of a suture passer through the clavicle from anterior to posterior after creating a drill hole in the superior and anterior clavicle. It is important not to tie the suture or repair the coracoclavicular ligaments just yet, as this will be done only after satisfactory reduction. This reduction is aided with the help of a Bristow elevator placed superior and medial to the fracture. The reduction is maintained manually with downward pressure or the use of a small fragment bone-holding clamp. The reduction is preferably stabilized with a four- or five-hole pelvic reconstruction plate affixed to the clavicle in the standard AO/ASIF technique. It is important to ensure that the distal fracture fragment can support at least four cortices before proceeding with plate fixation. If this does not seem possible, use a six-hole small fragment T-shaped plate for fixation or two Kirschner wires and a tension band technique. Two 0.062-inch Kirschner wires are drilled through the medial aspect of the distal fragment exiting posterolaterally. These wires are then passed anterograde through the distal fragment into the proximal fragment while the fracture is held reduced. A tension band is then placed around the wires and through an anterior to posterior drill hole in the proximal fragment. We prefer Arthrex Fiberwire (Naples, FL) as the tension band because of its low profile and strength. Fiberwire has been shown to exceed peak load and knot break strength of Ethibond number 5 (Ethicon, Somerville, NJ). The ends of the Kirschner wires are bent to deter migration, and the sutures in the coracoclavicular ligaments are tied. The Mersilene tape is then tied with multiple surgeon’s knots. The wound is thoroughly irrigated. Prior to the closure, we prefer to place a pain pump at the site of repair to aid in postoperative pain management. The wound is then closed in layers, taking care to preserve the deltoid and trapezial fascia. Using horizontal mattress sutures of number 1 or 0 nonabsorbable suture, the surgeon next closes the fascia over the clavicle. Any split in the deltoid muscle fibers should be closed at this time with 0 absorbable suture. The subcutaneous layer is closed with 3-0 monocryl. The skin is closed with a 4-0 monocryl subcuticular stitch for cosmesis. The incision is supplemented with steri-strips. The wound is then dressed with 4-inch by 4-inch pads and foam tape. A Cryocuff (Aircast, Summit, NJ) is placed over the dressed wound, and the upper extremity is immobilized in a shoulder immobilizer. The patient returns to the office postoperatively on day 2 for dressing change and pain pump removal. Strengthening and active range of motion exercises of the hand and elbow begin at that time. The skin sutures are removed in 7 to 10 days. The patient is permitted to use the elbow and hand for activities of daily living. The glenohumeral joint is kept continuously immobilized for 6 weeks in a sling. This is in contrast to current thought about rehabilitation of the shoulder girdle. However, because this is a procedure that spares the glenohumeral joint, early range of motion is not indicated. The patient is also restricted to no more than 5 pounds of pushing, pulling, or carrying. After radio-graphic evidence of healing, Kirschner wires, if used, are removed at 6 to 8 weeks. Prior to that, we see the patient no less frequently than every 2 weeks with x-rays to check for any Kirschner wire migration. At 6 to 8 weeks postoperatively, with signs of radiographic healing, the patient begins active assisted range of motion of the shoulder girdle to include forward flexion, abduction, and internal and external rotation. Only after radio-graphic evidence of healing is rotator cuff and deltoid strengthening begun. Physical therapy is advanced as solid radiographic healing becomes evident. After solid clinical and radiographic union is observed, the patient is advanced to full range of motion and full active use of the extremity. We allow the patient to return to unrestricted work or athletic activities when full active unrestricted range of motion of the shoulder is not painful. This usually occurs within 6 months of the surgical procedure. These injuries usually occur in sports that expose the competitor to a direct downward blow onto the lateral aspect of the shoulder. As such, a large number of these patients are younger males in their second decade who participate in football, hockey, and rugby. Probably the most commonly employed classification of AC joint injuries is that of Rockwood et al,2 whose six categories of injury follow a spectrum of severity in the sequence of failed structures. A description of these injuries typically departs from the standard convention of referring to the direction of displacement of the distal fragment. Instead, the displacement of the clavicle relative to the acromion determines the direction and type of dislocation. At the least, radiographic evaluation of these injuries should include AP and axillary views of the shoulder.
Distal Clavicle Fractures and Acromioclavicular Joint Injuries
Anatomy and Biomechanics
Distal Clavicle Fractures
Incidence
Classification
Treatment
Nonoperative Treatment
Operative Treatment
Technique
Postoperative Care
Acromioclavicular Joint Injuries
Mechanism of Injury
Classification
Distal Clavicle Fractures and Acromioclavicular Joint Injuries
Only gold members can continue reading. Log In or Register to continue


Full access? Get Clinical Tree


