Fig. 8.1
Gross anatomy of the clavicle and mean cross-sectional dimensions (Modified Jeray [21]. April 2007 Copyright Lippincott Williams & Wilkins)
Micro-computed tomography can be used to depict the internal trabecular structure of the clavicle (Fig. 8.2). This image demonstrates thick cortices and a paucity of trabecular bone within the diaphysis as compared to the medial and lateral ends where the cortices are thinner and the trabecular density is greater. This internal structure is similar to the other long bones in the skeleton.
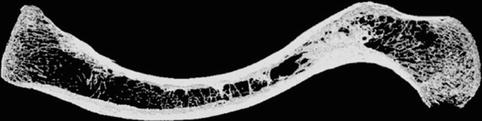
Fig. 8.2
Micro-CT scan of clavicle demonstrating trabecular and cortical bone patterns (Copyright Gregory Bain)
Four muscles arise from, and two muscles insert into, the clavicle. The deltoid arises from the anterior surface of the lateral curvature and the clavicular head of pectoralis major arises from the anterior aspect of the medial curvature. There is a small hiatus between these two origins although this is difficult to discern during surgery. The clavicular head of sternocleidomastoid arises from the posterior aspect of the medial curve opposite pectoralis major. Just medial to the sternocleidomastoid is the origin of the clavicular part of sternohyoid. The trapezius is the major muscle inserting onto the clavicle. It does so opposite the deltoid on the posterior aspect of the lateral curvature. The subclavius has a fleshy insertion on the inferior aspect of the middle third at the subclavian groove. It is worth noting that subclavius is the only muscle that has its main attachment in the middle third of the clavicle. The relative paucity of soft tissue attachments in the middle third may have an influence on the incidence of fractures in this region and certainly influences the deformity after fracture.
8.3 Vascularity and Related Neurovascular Structures
Two cadaveric studies have demonstrated that the clavicular blood supply is predominantly periosteal with only sporadic, very short intra-osseous arteries in a few specimens [6, 7]. In contrast, Crock demonstrated that there are some nutrient vessels running within the clavicle as was evident on anatomic specimens with the periosteum removed [8] (Fig. 8.3). The main arterial supply came from branches of the thoracoacromial artery and suprascapular artery. The internal mammary artery also gave a contribution in one study. The periosteal blood supply was always on the anterior and superior surfaces of the clavicle and concentrated in the middle third of the bone. There was never any periosteal supply on the posterior or inferior surfaces. The lack of periosteal supply substantiates the increased risk of non-union in high-energy mid-shaft fractures where periosteal stripping and wide displacement of the bony ends occurs. It also highlights the importance of surgical technique when dissecting the anterior-superior aspect of the clavicle for plate fixation.

Fig. 8.3
Arterial supply of the clavicle. The nutrient artery is well seen in this specimen. Note the predominant periosteal blood supply, as has been identified by other authors [8] (Copyright HV Crock AO)
The subclavian artery and vein, and the divisions of the brachial plexus, lie posterior to the medial curvature of the clavicle and pass beneath the middle third of the clavicle where the divisions branch into cords and the subclavian vessels become the axillary vessels. Cadaveric data has demonstrated the subclavian vein to lie directly beneath the middle and medial third junction with the left subclavian vein marginally more medial than the right [2]. The subclavian artery lies lateral to the vein but is still medial to the midpoint of the clavicle. Both vessels are separated from the bone by the subclavius muscle although this muscle is fleshy and frequently torn in traumatic injuries. The median distance from the superior aspect of the clavicle to the subclavian artery in an intact clavicle was 26.1 mm (range 22–34 mm) [2].
Just proximal to the clavicle, the anterior and posterior divisions of the brachial plexus form the medial, lateral and posterior cords named after their relationship to the axilliary artery. Indeed, clavicular osteotomy can be performed to expose the plexus at this level. Of all the branches of the brachial plexus, the medial cord, which goes on to form the ulnar nerve, is closest to the middle and medial third junction and is hence the most commonly injured peripheral nerve in a clavicle fracture. The posterior and lateral cords lie posterior and lateral to the axillary artery, where they are relatively shielded.
Although the neurovascular structures are in close proximity to the medial half of the clavicle, they are protected from the bone by a continuous myofascial tissue layer extending from the omohyoid fascia in the neck down to the clavipectoral fascia which encases the pectoralis minor and subclavius muscles [9]. This layer is evident in comminuted fractures and retained in non-unions. Careful development of this plane is possible and recommended in all clavicle surgery in order to protect the adjacent neurovascular structures.
8.4 Function
The bony geometry of the shoulder girdle has developed and adapted according to the requirements of different species. A pronounced variation amongst mammals is the presence or absence of the clavicle. Mammals adapted for running and swimming such as horses or whales have lost their clavicle, which allows greater motion of the scapula. Mammals that fly have very long clavicles but a narrow small scapula. Humans and other brachiating mammals have strong well-developed clavicles and scapulae. This is an adaptation to perform tasks using the hands well away from the body and to climb, swing and grasp distant objects. These teleological differences help to define the function of the clavicle [4]. The primary role of the clavicle is to position the arm away from a trunk and provide a stable strut between the arm and the axial skeleton. Having a stable strut allows the muscles to generate adequate power to perform reaching and elevation tasks. In this way the clavicle behaves like the arm of a tower crane suspending the arm away from the body (Fig. 8.4). It is stabilized by the muscular and ligamentous attachments which are least yielding medially at the sternoclavicular ligaments. There is therefore relative rigidity of the clavicle medially compared to laterally, allowing the clavicle to rotate about its axis thereby working as a crankshaft to augment scapula motion. The scapula rotates a total of 60° during abduction of the arm [4]. Thirty degrees of this rotation comes purely from lateral clavicle rotation whereas the remaining 30° comes from angulation of the whole clavicle and scapula together at the sternoclavicular joint. The clavicle’s role as a strut is not only important for activities performed away from the body but also when the arm is adducted and brought back into the body or across the trunk. The strut provides a fixed pivot for the arm to rotate and move around, without which this motion would be uncoordinated and inefficient. The clavicle’s role as a strut for power generation and its role in range of motion have been questioned on the basis that some patients with severe shortening or even absence of the clavicle can have little functional deficit in arm elevation. However, other authors have reported weakness, fatigue, neurologic symptoms and inferior functional scores related to clavicular malunion with shortening [10]. The compensation seen in many patients with a clavicular abnormality may be related to the continuous myofascial sleeve that encircles the clavicle [9] although a stable bony framework to support these muscles must be mechanically advantageous and is likely to be more important in repetitive or heavy activities. Furthermore, the clavicle serves a protective role to the adjacent neurovascular structures. With shortening or malunion, these structures are more likely to suffer impingement and compromise as is often seen in non-unions and sometimes malunions [10] following fracture.

Fig. 8.4
The clavicle acts as a strut to suspend the limb away from the axial skeleton much like the arm of a suspension crane. See Chap. 39 for more detail
8.5 Clavicle Fractures
The clavicle is the most commonly fractured bone in the skeleton [4]. There are a variety of classification systems but most are based on the anatomic location of the fracture [4]. Eighty percent of fractures occur in the middle third of the bone. This is the region with the narrowest cross-sectional diameter and where compressive forces across the shoulder are concentrated [1]. In addition, the middle section has no muscular or ligamentous attachment, which makes it vulnerable to the bending moments exerted by the structures attached to the middle and distal thirds of the bone. Lateral third fractures occur in 15 % of cases. They are more common in elderly patients or those with co-morbidities, although they do occur in all age groups. Medial third fractures (5 %) are uncommon and are typically associated with high-energy trauma in middle-aged men [11]. Occult injuries to the thorax, spine and head should be searched for in these injuries.
The typical mechanism of injury leading to a fracture of the clavicle is a fall with direct impact to the outer aspect of the shoulder. In a middle third fracture, the lateral fragment is typically shortened, inferiorly translated and anteriorly rotated. The resultant uncoupling of the distal segment from the axial skeleton results in protraction of the scapula [1] (Fig. 8.5). The weight of the arm causes inferior displacement of the lateral fragment while the medial fragment is superiorly displaced by contracture of the sternocleidomastoid. The trapezius causes shortening due to its attachment on the distal fragment. These strong muscular forces and weight of the arm mean closed reduction and any form of sling immobilization is unsuccessful in reducing or maintain reduction of a middle third clavicle fracture.