Fig. 5.1
Posterior view right scapula, demonstrating the primary and secondary ossifications centers
5.2 Description of Structure
Oriented superior, anterior, and lateral to the axis of the scapula, the coracoid process comes off the scapula at the upper base of the neck of the glenoid and passes anteriorly before hooking to a more lateral position as it projects from the superior body of the scapula.
The coracoid process [8] showed in cadaveric study that the average length of the coracoid process is approximately 4.3 cm. The width and height at the tip is 2.1 and 1.5 cm, respectively (Table 5.1).
Table 5.1
Coracoid process dimensions
Variable | Mean | SD | Range |
|---|---|---|---|
Length (cm) | 4.3 | 0.3 | 3.8–4.6 |
Tip width | 2.1 | 0.2 | 1.8–2.4 |
Tip height | 1.5 | 0.1 | 1.2–1.7 |
The distance separating the clavicle and the superior coracoid is 1.1–1.3 cm.
No statistically significant correlations were found between length or thickness of the coracoid process, prominence of the coracoid tip, coracoid slope, coraco-glenoid distance, or position of the coracoid tip with respect to the uppermost point of the glenoid. These anatomical characteristics were independent of the dimensions of the scapulae.
Three configurations of the coraco-glenoid space were identified.
Type I – Round bracket 45 %
Type II Square bracket 34 %
Type III Fish hook 21 %
The lowest value of the coraco-glenoid distance were seen in Type I scapulae. Morphometric characteristics that might predispose to subcoracoid impingement were found in 4 % of Type I scapulae [9].
5.3 Muscle: Tendon Attachment
The coracoid process functions as origin of muscles and ligaments insertion (Fig. 5.2a, b).
Fig. 5.2
(a) Attachments into the left coracoid process. CAL coracoacromial ligament, CP coracoid process, CT conjoint tendon, CUL coracohumeral ligament, P Minor pectoralis minor, CC ligs, trapezoid and conoid ligaments (Used with permission from Di Giacomo [39]). (b) Attachments into the left coracoid process (Used with Permission from Last [40])
The ascending portion, flattened from before backward, presents in front a smooth concave surface, across which pass the Subscapularis.
The horizontal portion is flattened from above downward; its upper surface is convex and irregular and gives attachment to the pectoralis minor; its under surface is smooth; its medial and lateral borders are rough; the former gives attachment to the pectoralis minor and the latter to the coracoacromial ligament; and the apex is embraced by the conjoined tendon of origin of the Coracobrachialis and short head of the Biceps brachii and gives attachment to the coracoclavicular fascia.
On the medial part of the root of the coracoid process is a rough impression for the attachment of the conoid ligament, and running from it obliquely forward and lateralward, on to the upper surface of the horizontal portion, is an elevated ridge for the attachment of the trapezoid ligament [10].
In summary:
Pectoralis minor muscle – from 3rd to 5th rib
Short head of biceps brachii muscle – to radial tuberosity
Coracobrachialis muscle – to medial humerus
Coracoclavicular ligament (conoid ligament and trapezoid ligament) – to the clavicle
Coracoacromial ligament – to the acromion
Coracohumeral ligament – to the humerus
Superior transverse scapular ligament – from the base of the coracoid to the medial portion of the suprascapular notch
The distance of these structures to the tip of the coracoid is shown in Table 5.2.
Table 5.2
Ligament footprint: distance from coracoid tip
Variable | Mean | SD | Range |
|---|---|---|---|
Posterior CAL | 2.8 | 0.33 | 2.0–4.0 |
Conjoint tendon | 0.53 | 0.27 | 0.2–1.2 |
Anterior pect minor | 1.2 | 0.10 | 1.0–1.4 |
Posterior pect minor | 1.6 | 0.27 | 1.1–2.3 |
Conoid | 3.7 | 0.35 | 3.0–4.2 |
Trapezoid | 3.3 | 0.38 | 2.8–4.4 |
Coracohumeral ligament Coracohumeral ligament | 1.7 | 0.32 | 1.2–2.4 |
Although the coracoclavicular ligament complex functions as a single ligament, it is composed of two distinct ligaments.
The two coracoclavicular ligaments (conoid and the trapezoid) attach the coracoid to the distal end of the clavicle and have an average length of about 1.3 cm [11]. The distance from the lateral edge of the clavicle to the center of the trapezoid and conoid tuberosities was 2.6 ± 0.4 cm and 3.5 ± 0.6 cm, respectively [12]. Several biomechanical studies have recently examined the function of the conoid and trapezoid ligaments in human cadaveric models [13–15].
The coracoclavicular ligaments function to stabilize the clavicle to the scapula with the conoid ligament primarily preventing anterior and superior clavicular displacement. The trapezoid ligament is the primary constraint against compression of the distal clavicle into the acromion [13].
The trapezoid ligament (ligamentum trapezoideum), the anterior and lateral fasciculus, is broad, thin, and quadrilateral: It is placed obliquely between the coracoid process and the clavicle. It is attached, below, to the upper surface of the coracoid process; above, to the oblique ridge on the under surface of the clavicle. Its anterior border is free; its posterior border is joined with the conoid ligament, the two forming, by their junction, an angle projecting backward. The width of the clavicular origin of the trapezoid ligament was 1.2 ± 0.1 cm.
The conoid ligament (ligamentum conoideum), the posterior and medial fasciculus, is a dense band of fibers, conical in form, with its base directed upward. It is attached by its apex to a rough impression at the base of the coracoid process, medial to the trapezoid ligament; above, by its expanded base, to the coracoid tuberosity on the under surface of the clavicle, and to a line proceeding medial ward from it for 1.25 cm. The conoid width at its clavicular origin was 2.5 ± 0.5 cm. The broad conoid ligament was not reliably centered over the most prominent aspect of the conoid tuberosity.
These ligaments are in relation, in front, with the subclavius and deltoideus; behind, with the trapezius. The coracoclavicular ligaments perform two major functions: (1) They guide synchronous scapulohumeral motion by attaching the clavicle to the scapula and (2) they strengthen the AC articulation.
5.3.1 Blood Supply
The vertical part of coracoid process is supplied by suprascapular artery and the horizontal part by branches of the axillary artery [16].
The blood supply is derived from vessels in muscles that have fleshy origin from the scapula.
Vessels cross these indirect insertions and communicate with bony vessels. The circulation of the scapula is metaphyseal; the periosteal vessels are larger than usual, and they communicate freely with the medullary vessels rather than being limited to the outer third of the cortex. Such anatomy might explain why subperiosteal dissection is bloodier here than over a diaphyseal bone. The nutrient artery of the scapula enters into the lateral suprascapular fossa or the infrascapular fossa. The subscapular, suprascapular, circumflex scapular, and acromial arteries are contributing vessels.
This anatomical study has shown that the coracoid process had its own blood supply. During the Latarjet procedure, vascular sacrifices are mandatory to allow coracoid process transfer to the scapular neck. Such sacrifices could partially explain lysis or nonunion of the coracoid process after Latarjet procedure. Preservation of axillary artery branches supplying horizontal part of the coracoid process could be a possible solution to prevent nonunion and lysis of the bone transfer.
5.4 Variations
Several anomalies of the coracoid have been described. Pieper and colleagues [17] reported variations in the coracoacromial ligament in 124 shoulders. Their findings were two distinct ligaments in 60 % and one ligament in 26 % of shoulders. They were also able to identify a third band located more posterior and medial than the conoid in 15 % of shoulders. Very little variation was found in the dominant and nondominant shoulders of the same cadaver with regard to number of bands.
5.5 Imaging
The coracoid process is not easily visualized on a radiograph. Apart from the usual three-view trauma series, an AP tilt view (35° to 60°) and a Stryker notch view. A CT scan with three-dimensional reconstruction images will give more insight into the fracture pattern (Fig. 5.3).
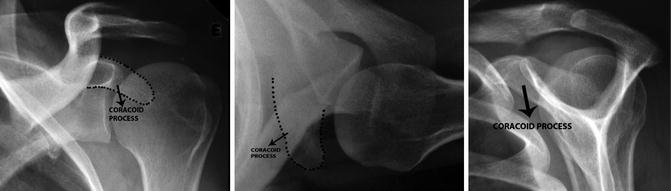
Fig. 5.3
Radiographs of normal left shoulder; AP axillary view and lateral views
5.6 Adjacent Structures
The coracoid process is readily palpable in the infraclavicular region just under the anterior head of the deltoid.
Lo et al. [18] showed that the portion of the coracoid tip which was closest to the neurovascular structures was the anteromedial portion of the coracoid tip. The distance from the anteromedial portion of the coracoid tip to each structure is as follows: axillary nerve 3.0 cm, musculocutaneous nerve 3.3 cm, lateral cord 2.9 cm, and axillary artery 3.7 cm. Similarly, the portion of the base of the coracoid that was closest to the neurovascular structures was its anteromedial portion. The shortest distance from the anteromedial aspect of the base of the coracoid to the axillary nerve, the musculocutaneous nerve, the lateral cord, and the axillary artery was 2.9, 3.7, 3.7, and 4.3 cm, respectively. Procedures about the coracoid are relatively safe procedures. The lateral cord of the brachial plexus is at greatest risk during dissection about the tip of the coracoid, and the axillary nerve is at greatest risk during dissection about the base of the coracoid. Pan et al. [19] demonstrated that the lateral cord moved closer to the coracoid process at 60° than at 30° of abduction under traction during simulated shoulder arthroscopy position using the lateral decubitus position.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


