CHAPTER 8 Arthroscopic Subacromial Decompression
Arthroscopic subacromial decompression (ASAD) has become one of the most commonly performed surgical procedures of the shoulder. The arthroscopic technique has evolved significantly from the open anterior acromioplasty as described by Neer1,2 and others, and the learning curve should not be underestimated.
ANATOMY AND PATHOANATOMY
Knowledge of the coracoacromial anatomy is crucial for diagnostic accuracy, operative facility, and avoidance of complications. The shape of the acromion and contour of its undersurface is best evaluated with Neer’s supraspinatus outlet view. Bigliani and colleagues3 have described three distinct acromial shapes: type 1, flat (divergent); type 2, curved (congruent); and type 3, hooked (stenotic). They found an increased correlation between the type 3 hooked acromion and underlying full-thickness rotator cuff tears (69.5% for type 3 and 3% for type 1). This radiographic view is also valuable for determining the overall slope and thickness of the acromion and in predetermining where and how much bone should be removed with acromioplasty, when indicated.
It is important to remember that the subacromial bursa is an anterior structure. It extends from the anterior half to one third of the acromion to just medial to the acromioclavicular (AC) joint to 1 to 2 cm anterior to the acromion and 2 to 3 cm laterally. The bursal wall is frequently thickened and troublesome posteriorly, and has been termed the posterior bursal curtain. This curtain frequently closes as one backs the arthroscope posteriorly to get a larger field of view of the subacromial bursa. It is frequently necessary to resect a portion of this structure when performing subacromial surgery.
The anatomy of the coracoacromial ligament (CAL) is pertinent to the technique of acromioplasty. It attaches to the front and undersurface of the acromion as a thick band and continues around the anterolateral corner to attach to the lateral ridge for a variable distance.4 Anteriorly, the posterior medial band of the coracoacromial ligament attaches to the anteroinferior edge of the acromion, whereas the deltoid fascia attaches more superiorly (Fig. 8-1).
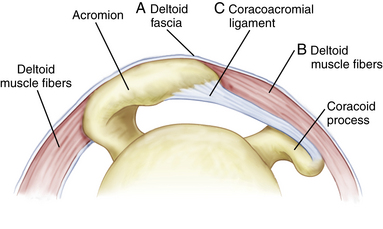
Anteriorly, the CA ligament attaches on the inferior acromial surface and falls away easily from the overlying anterior deltoid muscle and fascia when detached. Laterally, however, the anterior lateral band of the coracoacromial ligament blends inextricably with the deltoid muscle fascia along the lateral acromion.5 Care must be taken when releasing or ablating the anterolateral band of the CAL not to detach the fascia aggressively or resect too much bone laterally, because this may result in a deltoid detachment.
Edelson and Luchs6 and others have noted variable degrees of transformation of the coracoacromial ligament into bone at its acromial insertion, most commonly in the anterolateral band.4 Gartsman7 has labeled this phenomenon anterior acromial protuberance. Rockwood and Lyons,8 in their open technique, recommend resecting 8 to 10 mm of full-thickness anterior bone and then reattaching the deltoid fascia. This technique of full-thickness anterior bone resection back to the level of the AC joint has been included in a description of arthroscopic subacromial decompression.9
HISTORY AND PHYSICAL EXAMINATION
Causes of Impingement
Secondary Impingement
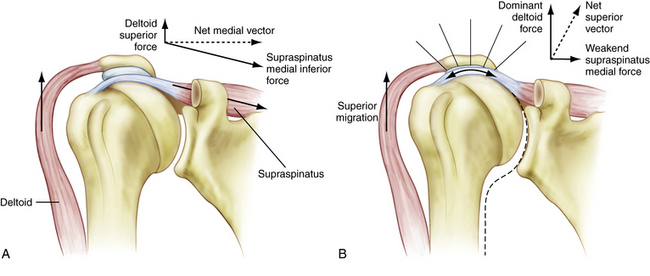
The concept of secondary impingement originated with Codman,10 who proposed an intrinsic tendinous degeneration as the essential lesion in rotator cuff disease. The microvascular studies of Rathbun and McNab11 and Moseley and Goldie12 support this concept. The subsequent pain and weakness of the supraspinatus compromises its function as a humeral head depressor and allows the superior vector forces of the deltoid to dominate, producing a secondary, superiorly directed impingement of the cuff into the acromion (Fig. 8-2 A, B).
Jobe and associates13 expanded this concept to include patients with underlying anterior glenohumeral ligament instability. As the humeral head subluxes anteriorly, the cuff is secondarily compressed against the coracoacromial arch. In addition, Matsen and coworkers14 have noted that posterior inferior capsular contracture produces an obligate anterior superior humeral head translation, with arm elevation and subsequent superior impingement.
Chronic Secondary Impingement with Pathologic Subacromial Changes
If the underlying cause of the secondary impingement is not rectified with a diligent rehabilitation program (e.g., scapular alignment, posterior capsule stretching), the cuff and humeral head elevate. The decreased acromial–humeral head distance results in inflammation and anterior mechanical irritation in the subacromial space, with the development of a traction spur in the acromial attachment of the CAL. This anterior acromial osteophyte formation can lead to awning impingement with arm elevation and subsequent bursal side cuff fraying and roughening. Even if subacromial space changes are present on a secondary basis, débridement, including a possible subacromial decompression, must be considered.
Primary Extrinsic Impingement
Neer1 introduced the concept of extrinsic impingement of the anterior acromion, coracoacromial arch, and AC joint on the underlying rotator cuff and biceps tendon. He also emphasized that forward flexion of the arm is the dominant functional position and that anterior decompression, not lateral acromionectomy, is the appropriate operative approach for significant cuff degeneration.
Neer’s impingement sign is determined with the patient seated in front of the examiner, who stabilizes the scapula as the arm is elevated slightly lateral to the midline to impinge the tuberosity against the acromion (Fig. 8-3).

Pain thus produced is eliminated by injecting 10 mL of 1% lidocaine (Xylocaine) into the subacromial bursa beneath the anterior acromion (impingement injection test) to confirm the diagnosis. Hawkins and Kennedy15 have described a second impingement sign, in which the arm is flexed forward 90 degrees and then forcibly internally rotated, jamming the supraspinatus tendon against the anterior edge of the coracoacromial ligament to produce pain (Fig. 8-4).

Posterior Superior Internal Impingement
Walch and colleagues16 and Jobe and associates17 have described a variety of secondary impingements noted in overhead athletes that occur when the arm is maximally externally rotated while abducted and extended, such as in the cocking phase of throwing. In this position, the posterosuperior articular surface fibers of the supraspinatus are placed under tension and shear but are also compressed between the humeral head and adjacent glenoid rim, resulting in posterior superior synovitis and partial undersurface tears.
Morgan and Rajan18 have described a subset of throwers with glenohumeral internal rotation deficit (GIRD). This posteroinferior capsular contracture produces a posterosuperior humeral head translation, superior labral separation, and internal impingement. Whether any underlying anterior instability is a factor in this type of compression needs to be determined with each individual case. In long-standing cases of internal impingement and superior labral pathology, obligate anterior instability can be encountered and may need to be addressed.
Anterior Subcoracoid Impingement
Gerber and coworkers19 have described this type of anterior impingement between the humeral head and coracoid process. The coracoid tip may be enlarged, fractured, or iatrogenically altered, such as occurs with a laterally positioned Bristow-Latarjet transfer of the coracoid tip onto the anterior glenoid rim. Fractures of the coracoid from the recoil of a rifle in hunters may heal with lateral displacement. These changes are best noted on axillary view x-rays or a computed tomography (CT) scan with the arm flexed 90 degrees and internally rotated.
Whatever the underlying cause, the tip of the coracoid is positioned more laterally than normal and, as the arm is brought into forward flexion, there is a compression of the anterior rotator cuff between the humeral head and tip of the coracoid. This produces pain with Neer’s forward flexion test, but it occurs usually between 80 and 130 degrees of flexion rather than at full flexion. Also, Hawkins flexion and internal rotation test is consistently positive, but the pain is lower and more anterior than with superior impingement. The patient also demonstrates decreased horizontal adduction, with pain similar to that found with AC disease (Fig. 8-5) but again, the pain is more at the tip of the coracoid and not at the AC joint. Selective injections in the region of the coracoid process can help verify the diagnosis.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


