Chapter 18 Amputations of the Upper Extremity
Amputations should be considered the start of rehabilitation. Major amputations of the upper extremity (other than digital amputations) account for 3% to 15% of all amputations and are approximately 20 times less common than amputations of the lower extremity. Trauma is the most common reason for upper extremity amputations except for shoulder disarticulation and forequarter amputations, for which malignant tumors are the primary reasons. Generally, all possible length should be preserved in upper extremity amputations. Length preservation can be maintained by careful evaluation and lengthening of a short stump by distraction osteogenesis (the method of Ilizarov) and microvascular anastomosis. Distal-free flaps and spare-part flaps (fillet flaps) from the amputated limb also should be used to preserve length. However, prosthetists are able to fit even small stumps with prostheses to improve function. Often a small stump distal to the elbow can be functionally better than a long above-elbow amputation. A prosthetic limb cannot adequately replace the sensibility of the hand, and the function of a prosthetic limb decreases with higher levels of amputation. Few patients with amputations around the shoulder are regular prosthetic users. The use of a rigid dressing and subsequent early temporary prosthetic fitting in patients with transhumeral or more distal amputations encourages the resumption of bimanual activities, softens the psychological blow of limb loss, and decreases the prosthetic rejection rate. After 4 to 6 weeks postoperatively the soft tissues have healed significantly and the edema should be controlled enough to proceed with a definitive socket for the patient. A myoelectrical prosthesis may be an option for patients with a below-elbow amputation. However, in manual workers a more traditional device should be employed. Some institutions use hybrid systems consisting of a locking shoulder joint with a body-powered elbow and externally powered wrist and terminal devices. These systems are most useful in amputations of the dominant extremity. Recipients use the prosthesis for approximately 14 hours a day. Some reports indicate, however, that 50% of patients discontinue the use of the prosthesis after 5 years. Various terminal devices are available and are easily interchanged (Fig. 18-1). Regardless, experienced prosthetists are invaluable in ensuring that patients have proper functional devices, and they should be consulted, when available, for each patient.

Wrist Amputations
Amputation at the Wrist







Disarticulation of the Wrist
 Fashion a long palmar and a short dorsal skin flap (Fig. 18-2A). Begin the incision 1.3 cm distal to the radial styloid process, carry it distally and across the palm, and curve it proximally to end 1.3 cm distal to the ulnar styloid process.
Fashion a long palmar and a short dorsal skin flap (Fig. 18-2A). Begin the incision 1.3 cm distal to the radial styloid process, carry it distally and across the palm, and curve it proximally to end 1.3 cm distal to the ulnar styloid process.

 Just proximal to the joint, identify, ligate, and divide the radial and ulnar arteries.
Just proximal to the joint, identify, ligate, and divide the radial and ulnar arteries.

 At a proximal level, divide all tendons and allow them to retract into the forearm.
At a proximal level, divide all tendons and allow them to retract into the forearm.
 Incise the wrist joint capsule circumferentially, completing the disarticulation (Fig. 18-2B and C).
Incise the wrist joint capsule circumferentially, completing the disarticulation (Fig. 18-2B and C).
 Resect the radial and ulnar styloid processes, and rasp the raw ends of the bones to form a smoothly rounded contour. Take care to avoid damaging the distal radioulnar joint, including the triangular ligament, so that normal pronation and supination of the forearm are preserved and pain in the joint is prevented (Fig. 18-2D).
Resect the radial and ulnar styloid processes, and rasp the raw ends of the bones to form a smoothly rounded contour. Take care to avoid damaging the distal radioulnar joint, including the triangular ligament, so that normal pronation and supination of the forearm are preserved and pain in the joint is prevented (Fig. 18-2D).
 With interrupted nonabsorbable sutures, close the skin flaps over the ends of the bones (Fig. 18-2E), and insert a rubber tissue drain or a plastic tube for suction drainage.
With interrupted nonabsorbable sutures, close the skin flaps over the ends of the bones (Fig. 18-2E), and insert a rubber tissue drain or a plastic tube for suction drainage.
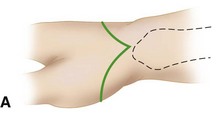
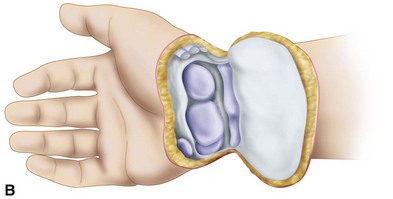



FIGURE 18-2 Disarticulation of the wrist. A, Skin incision. B and C, Reflection of the palmar flap and section of wrist joint capsule. D, Resection of tips of radial and ulnar styloids with preservation of the triangular ligament and underlying joint space. E, Completed amputation. SEE TECHNIQUE 18-2.
Forearm Amputations (Transradial)
Distal Forearm (Distal Transradial) Amputation
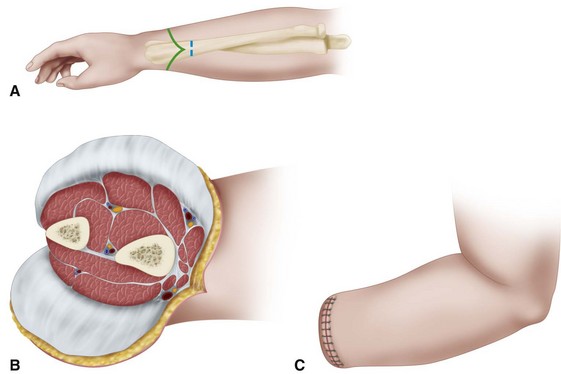
 Beginning proximally at the intended level of bone section, fashion equal anterior and posterior skin flaps (Fig. 18-3A); make the length of each about equal to one half of the diameter of the forearm at the level of amputation. Together with the skin flaps, reflect the subcutaneous tissue and deep fascia proximally to the level of bone section.
Beginning proximally at the intended level of bone section, fashion equal anterior and posterior skin flaps (Fig. 18-3A); make the length of each about equal to one half of the diameter of the forearm at the level of amputation. Together with the skin flaps, reflect the subcutaneous tissue and deep fascia proximally to the level of bone section.
 Clamp, doubly ligate, and divide the radial and ulnar arteries just proximal to this level.
Clamp, doubly ligate, and divide the radial and ulnar arteries just proximal to this level.


 Divide the radius and ulna transversely, and rasp all sharp edges from their ends (Fig. 18-3B).
Divide the radius and ulna transversely, and rasp all sharp edges from their ends (Fig. 18-3B).
 Close the deep fascia with fine absorbable sutures and the skin flaps with interrupted nonabsorbable sutures (Fig. 18-3C), and insert deep to the fascia a rubber tissue drain or, if preferable, a plastic tube for suction drainage.
Close the deep fascia with fine absorbable sutures and the skin flaps with interrupted nonabsorbable sutures (Fig. 18-3C), and insert deep to the fascia a rubber tissue drain or, if preferable, a plastic tube for suction drainage.

 Divide the remaining soft tissues transversely at the level of bone section.
Divide the remaining soft tissues transversely at the level of bone section.


Proximal Third of Forearm (Proximal Transradial) Amputation
 When good skin is available, fashion anterior and posterior skin flaps of equal length; if good skin is unavailable, fashion atypical flaps as necessary rather than amputate at a more proximal level. Reflect proximally to the level of intended bone section the deep fascia together with the skin flaps.
When good skin is available, fashion anterior and posterior skin flaps of equal length; if good skin is unavailable, fashion atypical flaps as necessary rather than amputate at a more proximal level. Reflect proximally to the level of intended bone section the deep fascia together with the skin flaps.
 Just proximal to this level, identify, doubly ligate, and divide the major vessels.
Just proximal to this level, identify, doubly ligate, and divide the major vessels.








